Approximately 13-44% of lung cancer patients develop central nervous system (CNS) metastasis; 50-60% of CNS metastases are from lung cancer. The incidence of CNS metastasis is rising, because patients are currently living longer and there is a better detection of metastasis using MRI [1,2].
Is there still a role for surgery?
Factors favouring intensified local therapy are the presence of a single or solitary metastasis, adequate performance status, no or mild neurological deficits, no or stable (>3 months) extracranial tumour manifestations, and the presence of a radioresistant tumour. “Apart from logical reasoning there is hardly any evidence that surgery of brain metastasis makes any sense”, Prof. Michael Weller (University Hospital Zurich, Switzerland) mentioned. “However, old data suggests that surgery for single metastasis prolongs survival.”
The factors favouring surgery over radiosurgery are in his view “collapsing”. The presence of an unknown primary tumour and neuroradiologically uncertain lesion are good reasons to perform an operation. Prof. Weller is critical about two other, frequently mentioned reasons in favour of surgery: the presence of a surgically accessible lesion and acceptable surgical risk. “Surgeons often say: if the lesion is accessible, you should take it out. But that is not really evidence. Simply the fact that you can do something, does not mean that you have to do that.”
Surgery has the advantage of delivering a tissue-based diagnosis, which avoids misdiagnosis and facilitates targeted therapy. Furthermore, surgery may allow for more rapid neurological improvement than any other anti-cancer treatment and remains the only effective treatment for large brain (oligo)metastasis.
- Li YS, et al. J Thorac Oncol. 2016;11:1962-1969.
- O'Kane GM, Leighl NB. CNS Drugs. 2018;32:527-542.
Posted on
Table of Contents: ELCC 2019
Featured articles
Electromagnetic navigation bronchoscopy
Current Management of Early Stage NSCLC
Trial Data: Early Stage Lung Cancer
Electromagnetic navigation bronchoscopy
Genomic and immune profiling
Immunotherapy in Stage 4 Lung Cancer
Other I-O combinations
Predictive diagnostics for I-O
Trials: Immunotherapy in Stage 4 Lung Cancer
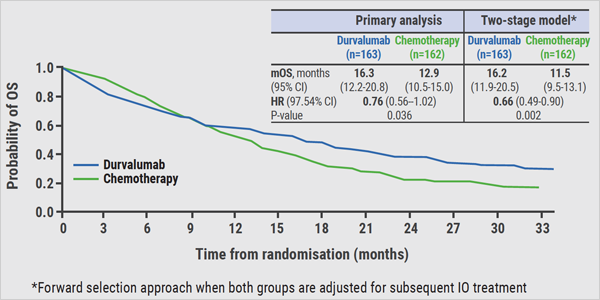
Post-study immunotherapy in MYSTIC
Implementation of Personalised Lung Cancer Care in Clinical Routine
How can societies help to implement personalised treatment?
Optimal Management of Brain Metastases in NSCLC
Incidence and local treatment
Brain irradiation as treatment option
Small Cell Lung Cancer: New Targets
Molecular characteristics of SCLC
Immunotherapy in SCLC: trial data
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com