This intervention has been evaluated in the global NAVIGATE study, the largest prospective, multicentre ENB study carried out, comprising diverse users and a challenging patient population (67% with bronchus sign, 54% lesions <20 mm, and 73% peripheral lesions). A previous 1-month interim analysis of the first 1,000 subjects who were enrolled in the primary cohort demonstrated low adverse event rates in a generalisable population across diverse practice settings [1].
A recent analysis presented by Dr Kelvin Lau (St Bartholomew’s Hospital, London, United Kingdom) at the ELCC meeting evaluated ENB safety and usage in the NAVIGATE European sites [2]. The results from the European cohort of the NAVIGATE study suggest that ENB provides a safe platform to aid in lung lesion biopsy. There was a low complication rate (5% pneumothorax requiring intervention) despite the challenging patient population. The median procedure time was only 40 minutes in total and 29 minutes for ENB navigation and sampling. Taken together, according to Dr Lau, this study suggests that ENB safety allows lung lesion biopsy, fiducial placement, and lymph node sampling during a single anaesthetic event [2].
In her own practice in the Netherlands, CT-guided biopsies are performed by the radiologist in case of a lung nodule, said invited discussant Dr Anne-Marie Dingemans (University Hospital Maastricht, the Netherlands). “In most cases, this intervention is successful. The pneumothorax rate in our hands is very low. So, what is the additive value of ENB in peripheral nodules?” Pulmonologists have a lot of tools for the diagnosis of small nodules, such as conventional bronchoscopy, ENB, ultrasound-guided bronchoscopy, endo-bronchial ultrasound (EBUS), CT-guided transthoracic needle aspiration (TTNA), and surgery. Dr Dingemans mentioned some pros and cons of these techniques: “Bronchoscopy is available everywhere, but sensitivity is probably low. ENB is useful for peripheral lesions, while EBUS is more interesting for staging of mediastinal lymph nodes. CT-guided biopsies have low cost, it is in my view safe and the sensitivity is very high in good hands, i.e. performed by an expert radiologist. Furthermore, you don’t need a bronchoscope to go to the nodule, which is an advantage of this technique. Surgery is more invasive, although I think no really risky things happen, but the sensitivity and specificity are the highest of all.”
A systematic review and meta-analysis, published in 2014, showed that ENB has a diagnostic yield of 65% for the detection of lung nodules. In case of a bronchial sign, the diagnostic yield is very high (79%) [3]. The NAVIGATE study is a post-market study to collect real world outcome data. In the analysis of the first 1,000 patients, the pneumothorax (CTCAE grade ≥2) rate was around 3.2% [1]. “This means that this is a very safe procedure”, concluded Dr Dingemans. “In the European cohort [2], there was a bronchial sign on the CT scan more frequently, so this is a better selection of patients who are suitable for this intervention compared with the overall cohort. The pneumothorax rate in the European cohort [2] was somewhat higher (5.1%), probably because the technique was used in more peripheral lesions.” In conclusion, while ENB is safe and it is possible to access all disease areas, it frequently requires general anaesthesia, you need a bronchial sign, and there are costs.
- Khandhar SJ, et al. BMC Pulm Med. 2017;17:59.
- Lau K, et al. ELCC 2019, abstract 68O.
- Gex G, et al. Respiration. 2014;87:165-76.
Posted on
Table of Contents: ELCC 2019
Featured articles
Electromagnetic navigation bronchoscopy
Current Management of Early Stage NSCLC
Trial Data: Early Stage Lung Cancer
Electromagnetic navigation bronchoscopy
Genomic and immune profiling
Immunotherapy in Stage 4 Lung Cancer
Other I-O combinations
Predictive diagnostics for I-O
Trials: Immunotherapy in Stage 4 Lung Cancer
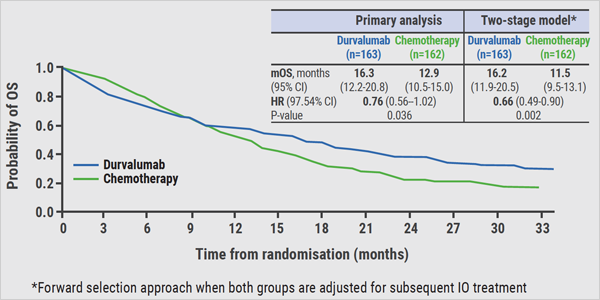
Post-study immunotherapy in MYSTIC
Implementation of Personalised Lung Cancer Care in Clinical Routine
How can societies help to implement personalised treatment?
Optimal Management of Brain Metastases in NSCLC
Incidence and local treatment
Brain irradiation as treatment option
Small Cell Lung Cancer: New Targets
Molecular characteristics of SCLC
Immunotherapy in SCLC: trial data
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy