
Migraine, a condition affecting more women than men, affects approximately 15% of the population during their most productive periods of their lives. The migraine brain is altered structurally and functionally with many neuronal systems functioning abnormally (i.e. generalised neuronal hyperexcitability). Migraine attacks often begin with a prodromal phase and an aura accompanied by transient focal, cortically mediated, neurological symptoms, developing gradually and resolving completely. Symptoms may include throbbing headache, nausea, vomiting, photophobia, abnormal sensitivity to noise and smell, allodynia, paraesthesia, and numbness (when the somatosensory cortex is affected), tremor and unilateral muscle weakness (when the motor cortex or basal ganglia are affected), and aphasia (involvement of speech area). The aura phase may last 5 minutes to 1 hour per aura type. The whole headache attack may last between 4 and 72 hours. Peripheral sensitisation is responsible for throbbing pain, while central sensitisation in the spinal cord mediates skin hypersensitivity and muscle tenderness. Sensitisation of thalamic trigeminovascular neurons results in whole-body allodynia. Cortical spreading depression - with a slowly propagating wave of alternating neuronal depolarisation and hyperpolarisation, vascular constriction, and dilation - is a neurovascular event underlying migraine aura.
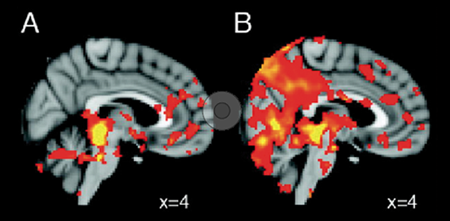
Episodic migraine patients do respond to triptan if treated early enough in the attack before establishment of central sensitisation. Chronic migraine patients, after establishment of central sensitisation, however, do not respond to 5-hydroxytryptamine (5-HT)1B/1D receptor agonists, the current standard acute treatment for migraine (Figure 1). The reason for this is that, as the disease progresses, the chronic state of central sensitisation leads to interictal allodynia and background headache, Prof. Burstein explained the underlying mechanism.
Figure 1: Lessons learned from triptan therapy in episodic and chronic migraine [1]

- Burnstein R, et al. Ann Neurol. 2004 Jan;55(1):19-26.
Posted on
Table of Contents: TOXINS 2019
Featured articles
Pain
Pain subsides before effect on muscles become apparent
Migraine
Central and peripheral mechanisms in migraine
Predictors of response
Spasticity
Why treat spasticity?
ASPIRE: High patient and clinician satisfaction
Cervical Dystonia
Anterocollis posture and deep cervical muscle injections
Daxibotulinum toxin in isolated cervical dystonia
Parkinson
Utility of botulinum toxin in Parkinson’s disease beyond sialorrhea
New Versions of Botulinum Toxins
New Versions of Botulinum Toxins
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com