The key take-home messages were (1) if minimal residual disease (MRD) negativity is achieved after CAR-T cell therapy, the majority of patients will be cured; (2) allogenic transplantation after CAR-T cell therapy grants patients an even better survival; (3) success of CAR-T cell therapy seems to be mostly dependent on the post-infusion expansion of CAR-T cells; and (4) the challenges, such as cytokine release syndrome (CRS) or CD19-negative relapse, require internationally coordinated homogeneous criteria.
The pivotal single-arm phase 2 ELIANA study infused 63 heavily pre-treated patients (half had had one or more stem cell transplantations) and showed >80% complete response (CR) including MRD negativity. This study placed CAR-T cells firmly in the spotlight as a novel therapeutic modality. Most of the first studies focussed on children and young adults <25 years old. Collectively, although the numbers are small, the consistent CR rate of 80-90% across studies, coupled with the fact that the majority of patients will proceed to MRD negativity, suggests that CAR-Ts can offer long-term survival in many patients (see Table for overview of all CAR-T trials in ALL). It also became evident that the use of CAR-T cells is associated with some severe and serious complications, namely cytokine release syndrome (CRS) and neurotoxicity; at least one-third of the patient will experience severe CRS, and another 25-33% will experience neurotoxicity [2].
Table: Overview of all CAR-T studies performed to date in ALL patients [1] CR, complete response; CRES, CAR-T related encephalopathy syndrome; CRS, cytokine release syndrome; MRD-neg, negative for minimal residual disease.
CR, complete response; CRES, CAR-T related encephalopathy syndrome; CRS, cytokine release syndrome; MRD-neg, negative for minimal residual disease.
In the study with the longest follow-up (median follow-up 29 months), older patients (up to 60 years) also demonstrated that more than half of ALL patients -despite their age- will achieve CR and MRD negativity [3]. This outcome appears to be dependent on the in vivo expansion of the CAR-T cells; using a lymphodepletion regimen based on fludarabine and cyclophosphamide is important to create the right environment to allow the expansion of the CAR-T cells, supported by co stimulatory molecules 4-1BB and CD28.
What are the factors associated with durable event-free survival after CAR-T cells in adult ALL? Hay and colleagues recently published their trial FH2639, a phase 1-2 study of defined composition CD19 XAR-T cells for relapse/refractory B-cell malignancies [4]. Forty-five of the 53 treated patients went into MRD-negative CR (85%). The take-home message from the ALL cohort of this paper was that the number of prior lines of therapy affects the outcome, i.e. the worse the disease burden, the worse the outcome. The most predictive value that came out of this study was the level CAR-T expansion after infusion. In contrast to what we hear about from lymphoma or myeloma, ALL patients can have a robust and long-term expansion of CAR-T cells. In terms of survival, the vast majority of MRD-negative patients appear to be cured, with a mean follow-up of 30.9 months. Although these data are a bit controversial, most data support that patients who received a transplant after CAR-T cells have a better 24-month survival (P=0.014) survival.
There are 2 major challenges:
- Toxicities. The symptoms frequently observed in CRS are fever, hypotension, capillary leak, coagulopathy, multi-organ failure, and MAS/HLH. Among the neurological toxicities we observe headaches, confusion, delirium, seizures, and focal/non focal deficits. The learning curve has improved management and timely intervention for these. Importantly, measures are being taken to create consensus within and among professional societies on how best to diagnose and treat CRS [5,6] adopting homogeneous criteria.
- Duration of response is determined by a lack of long-term persistence of CAR T cells. Around 80-90% patients achieve MRD negativity but only about 50% achieve a cure. One explanation for this discrepancy is the lack of persistence. In addition, up to 20% of ALL patients receiving CD19-specific CAR T cells will experience a CD19-negative relapse after CAR-T cell therapy. Possible mechanisms of loss of CD19 frameshift mutations clustered in CD19 exon 2 leading to expression of the Δex2 isoform not recognised by CAR-T cells [7]. Alternatively, it has been postulated that a full myeloid switch can occur in an MLL-rearranged ALL patient, which has been modelled in mice as well [8].
Prof. Mohty concluded, “We still hesitate about the positioning of CAR-T therapy within the ALL treatment, even ignoring accessibility and affordability aspects. Assuming all options are available, the question should be which strategy/algorithm? Should this be an option for consolidation in lieu of SCT? Or perhaps as a bridge to ASCT? Or as salvage therapy after ASCT (half of the patients receiving CAR T cells underwent ASCT)? How should we sequence with blinatumomab, inotuzumab, or combinations? Should we treat CRS pre-emptively with early intervention tocilizumab? When it comes to duration of response, optimisation of CAR T cell functionality should be researched, in particular in vivo persistence. Furthermore, immunogenicity reduction should be achievable with human/humanised scFv because antibodies can be detected against the murine construct.”
- Mohty M. 24th Congress of the EHA, 13-16 June 2019, Amsterdam, the Netherlands.
- Jackson HJ, et al. Nat Rev Clin Oncol. 2016 Jun;13(6):370-83.
- Park JH, et al. N Engl J Med. 2018 Feb 1;378(5):449-459.
- Hay KA, et al. Blood. 2019 Apr 11;133(15):1652-1663.
- Lee DW, et al. Biol Blood Marrow Transplant. 2019 Apr;25(4):625-638.
- Kansagra AJ, et al. Bone Marrow Transplant. 2019 May 15.
- Sotillo E, et al. Cancer Discov. 2015 Dec;5(12):1282-95.
- Gardner R, et al. Blood. 2016 May 19;127(20):2406-10.
Posted on
Table of Contents: EHA 2019
Featured articles
Editor Biography
Interview with EHA President Prof. Pieter Sonneveld
Myeloid Malignancies
Residual disease in AML patients prior to stem cell transplant increases relapse risk
Gilteritinib prolongs overall survival in patients with FLT3-mutated relapsed/refractory AML
Initial data on AMV564 in patients with relapsed/refractory AML
Overcoming the “don’t eat me” signal in AML and MDS
Asciminib plus imatinib in patients with heavily pre-treated chronic myeloid leukaemia
Guadecitabine vs treatment of choice in AML
Lymphoid Malignancies
Unmutated IGHV as predictive factor for venetoclax/obinutuzumab benefit in frontline CLL
CAR-T cell therapy in ALL as breakthrough advance
Brentuximab vedotin continues to demonstrate superior clinical activity in classical Hodgkin lymphoma
Infectious complications mild and not common in patients receiving CAR-T therapy for diffuse large B cell lymphoma
Obinutuzumab/polatuzumab in follicular lymphoma
Exciting survival data for ibrutinib vs placebo in treatment-naïve, early-stage CLL
ASCEND study: Acalabrutinib improves progression-free survival in relapsed/refractory CLL
Venetoclax-obinutuzumab combination elicits high response rates in CLL
Myeloma
CASSIOPEIA trial: Phase 3 results of daratumumab + bortezomib/thalidomide/dexamethasone in multiple myeloma
Chimeric antigen receptor T cell therapy in multiple myeloma
Higher levels of treatment satisfaction without compromising efficacy: subcutaneous daratumumab in RRMM
Adding isatuximab to pomalidomide and dexamethasone improves PFS and ORR in RRMM
Subcutaneous daratumumab + cyclophosphamide, bortezomib, and dexamethasone in patients with newly diagnosed amyloid light chain amyloidosis
Venetoclax for multiple myeloma: effective but some safety concerns
Benign Haematology
New sickle cell drug voxelotor boosts levels of haemoglobin
Positive initial data evaluating the safety and efficacy of IMR-687 for treatment of sickle cell disease
Haematopoietic stem cell transplantation improves stroke risk in children with sickle cell anaemia
Early trial data shows positive results for treating anaemia in patients with end-stage renal failure
Bench-to-Bedside
Transformation of foetal haematopoietic stem and progenitor cells in the background of trisomy 21
Treating thalassemia twice, in mice
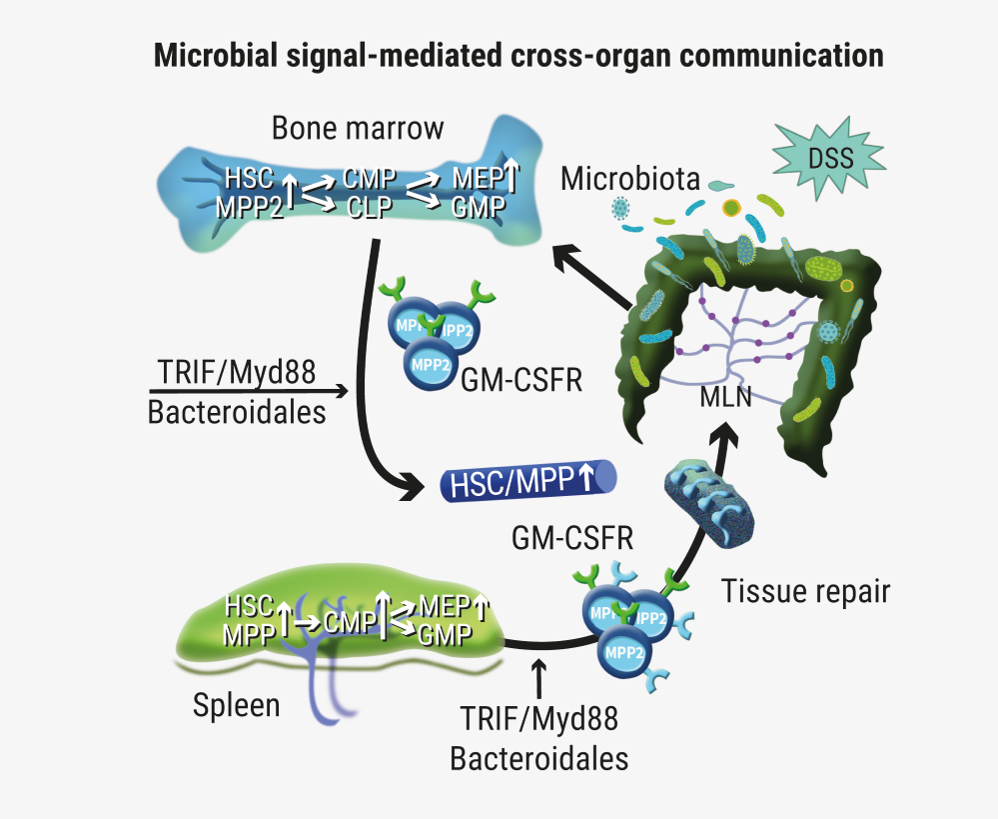
Haematopoietic stem cells can sense tissue damage in the gut
Promising news for gene therapy for sickle cell disease


site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy