Prof. Timothy Hughes (University of Adelaide, Australia) explained that asciminib binds a myristoyl site of the BCR-ABL1 fusion protein, locking BCR-ABL1 into an inactive conformation through a mechanism distinct from all other ABL kinase inhibitors [1]. Asciminib targets both native and mutated BCR-ABL1 fusion proteins, including the T315I-mutant fusion protein. The safety and clinical activity of asciminib in patients with Ph+ leukaemia are unknown.
Patients with Ph+ chronic phase or accelerated phase CML (n=48) were enrolled in an ongoing larger phase 1 study [2]. Patients who were relapsed/refractory or intolerant to ≥2 ABL tyrosine kinase inhibitors were assigned to 9 different oral asciminib dose cohorts (20, 40, 80, 150, 160, and 200 mg twice daily; 80, 120, and 200 mg once daily) evaluating asciminib alone or in combination with other therapies. The analysis presented by Prof. Hughes looked at the asciminib monotherapy cohorts with ≤1% BCR-ABL1 at baseline. Median duration of study treatment exposure was 161 weeks.
At data cut off, 36 patients (75.0%) manifested a major molecular response (MMR) or better, and median time to MMR among responders was 30 days. All 18 patients who achieved MMR maintained this for ≥2 years. Of the 6 patients who did not achieve MMR, 1 had baseline levels of BCR-ABL1 >1%, and 5 were between 0.1-1%.
The most common grade 3-4 adverse events (AEs), occurring in >10% of patients were lipase increases (27.1%) and hypertension (12.5%). Serious AEs were reported in 33.3% patients, and 2 patients experienced myocardial infarction (4.2%).
“In conclusion, asciminib monotherapy was well-tolerated and showed promising clinical activity in patients with baseline BCR-ABL1 levels less than 1%,” concluded Prof. Hughes during his presentation. “These results support further investigation of asciminib in patients who do not achieve optimal response at earlier time points.”
- Hughes T, et al. Asciminib in heavily pre-treated patients with Philadelphia chromosome-positive (Ph+) CML in chronic phase sensitive to TKI therapy. EHA25 Virtual, 11-21 June 2020, Abstract S170.
- Hughes TP, et al. Asciminib in Chronic Myeloid Leukemia after ABL Kinase Inhibitor Failure. N Engl J Med. 2019;381(24):2315-2326.
Posted on
Table of Contents: EHA 2020
Featured articles
Myeloid
VIALE-A: newly diagnosed chemo-ineligible AML
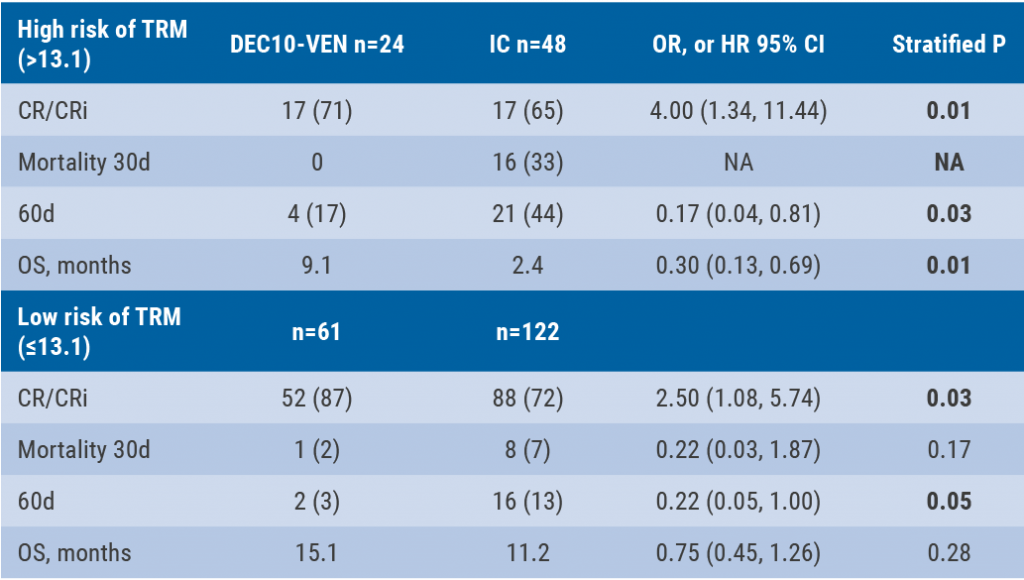
DEC10-VEN superior to intensive chemotherapy in high-risk AML
Magrolimab plus azacitidine: good ORR in MDS/AML
Asciminib monotherapy in Ph+ CML: major molecular responses
CML TKI interruption: Swedish registry results
Patients with lower-risk MDS benefit from imetelstat
Better outcomes adding enasidenib to azacitidine in mIDH2-AML
Lymphoid
PET-stratification can omit radiotherapy in early-stage unfavourable Hodgkin lymphoma
Pembrolizumab improves PFS for relapsed/refractory Hodgkin lymphoma
Promising first-in-human trial of epcoritamab in B-NHL
Two trials: acalabrutinib in CLL
Zanubrutinib versus ibrutinib in Waldenström macroglobulinaemia
Deep responses in R/R CLL with venetoclax monotherapy
MRD assessment post-CAR-T predicts ALL allo-HSCT bridging
Plasma Cell Dyscrasias
Daratumumab for light-chain amyloidosis
Isatuximab triplet improves PFS in R/R MM
Initial results from CAR-T cell therapy in MM: KarMMa
Graft-Versus-Host Disease
GRAVITAS-301: improved complete aGVDH response
Ruxolitinib improves steroid-refractory aGVHD across subtypes
Benign Haematology
Paroxysmal nocturnal haemoglobinuria treatment with pegcetacoplan
Mitapivat, a pyruvate kinase-R activator, in SCD is safe with early efficacy results
SCD LentiGlobin gene therapy: new data on VOC and ACS
Paediatric Haematology
Venetoclax + navitoclax promising for R/R ALL or LL
Nivolumab/brentuximab vedotin in R/R HL: good CMR rates
Bench-to-Bedside Science from the Presidential Symposium
Microbiome predicts B-ALL predisposition
Netrin-1 regulates haematopoietic stem cells
Unrecognised role of iron in neutrophil differentiation
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com