https://doi.org/10.55788/19ed7fb5
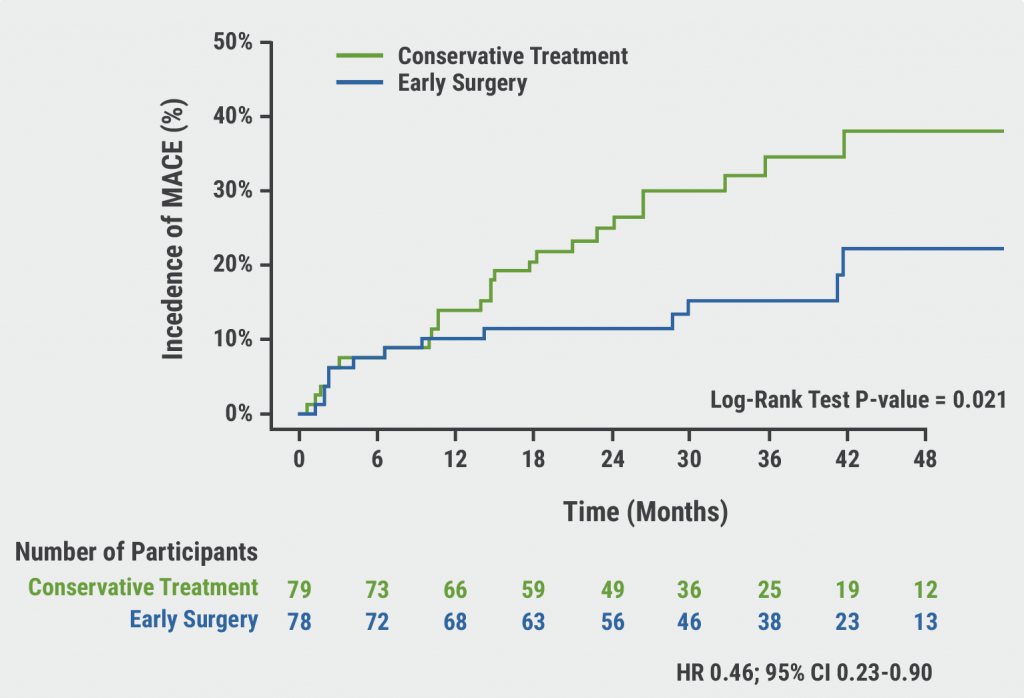
To date, it has not been thoroughly investigated whether a conservative or invasive strategy is the optimal management for patients with CKD and chronic coronary disease. To address this issue, the ISCHEMIA-CKD trial (NCT01985360) included 777 patients with CKD and moderate-to-severe ischaemia [1]. Participants were randomised to an initial invasive strategy for treating ischaemia, consisting of cardiac catheterisation and optimal revascularisation, either with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG), plus guideline-directed medical therapy, or to an initial conservative strategy, consisting of guideline-directed medical therapy and an invasive strategy, if medical therapy had failed.
After 2.2 years of follow-up, the primary results of the trial did not demonstrate a significant difference between the two treatment arms with respect to all-cause death, the primary outcome of the study [2]. Now, Prof. Sripal Bangalore (New York University School of Medicine, NY, USA) presented the results of the ISCHEMIA-CKD trial after 5 years of follow-up.
The death rate at 5 years was approximately 40%, indicating that the trial population consisted of very high-risk patients. No significant difference between an initial invasive strategy or an initial conservative strategy was reported at this 5-year interim analysis (adjusted HR 1.12; 95% CI 0.89–1.41; P=0.322). Likewise, no significant differences were observed for the secondary endpoints of cardiovascular death and non-cardiovascular death.
The final results of the trial are expected after a total of 9 years of follow-up.
- Bangalore S, et al. ISCHEMIA-CKD EXTEND – Clinical Outcomes at 5 years of Follow-up. Hot Line Session 8, ESC Congress 2022, Barcelona, Spain, 26–29 August.
- Bangalore S, et al. N Engl J Med. 2020;382:1608–1618.
Copyright ©2022 Medicom Medical Publishers
Posted on
Table of Contents: ESC 2022
Featured articles
ESC Clinical Practice Guidelines
Prevention of VT and sudden cardiac death: the new recommendations
New and first ESC cardio-oncology guideline
The 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension
Cardiovascular assessment and management of patients undergoing non-cardiac surgery
Heart Failure
Old dogs, new tricks: Acetazolamide plus loop diuretics improves decongestion
No effect of neprilysin inhibition on cognition
Dapagliflozin DELIVERs for HFmrEF/HFpEF
Meta-analysis of DELIVER and EMPEROR-Preserved
Anticoagulation
Rheumatic heart disease-associated AF: standard-of-care holds ground
New anticoagulant safe and maybe effective: PACIFIC-AMI and PACIFIC-Stroke outcomes
AXIOMATIC-SSP: Reducing risk of ischaemic stroke with factor XIa inhibition?
Evolving evidence for P2Y12 inhibition in chronic coronary syndromes: PANTHER
Prevention
Danish study suggests starting CVD screening before age 70
Polypill SECUREs win in secondary prevention in elderly
Long-term therapy with evolocumab associated with lower CV mortality
ARBs + beta-blockers may delay Marfan syndrome aortic root replacement
ENTRIGUE: Subcutaneous pegozafermin in severe hypertriglyceridaemia
Artificial Intelligence & Digital Health – What Is New
First RCT evidence for use of AI in daily practice
AI-enhanced echography supports aortic stenosis patients
Ischaemia
Medical therapy versus PCI for ischaemic cardiomyopathy
Allopurinol disappoints in ALL-HEART
Conservative or invasive management for high-risk kidney disease patients with ischaemia?
Genotype-guided antiplatelet therapy in patients receiving PCI
Other HOTLINE Sessions
BOXing out oxygen and blood pressure targets
Coronary CT angiography diagnostics compared head-to-head
High-dose influenza vaccine: mortality benefit?
FFR-guided decision-making in patients with AMI and multivessel disease
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com