
https://doi.org/10.55788/32ff9e8a
ET plus CDK4/6 inhibition is the standard-of-care for patients with HR-positive/HER2-negative metastatic breast cancer [1]. Although observational data supports switching ET while continuing CDK4/6 inhibitors after patients progress, no prospective, randomised trials have evaluated this approach [2]. The phase 2 MAINTAIN trial (NCT02632045), presented by Prof. Kevin Kalinsky (Winship Cancer Institute of Emory University, GA, USA) randomised 119 patients with HR-positive/HER2-negative metastatic breast cancer who progressed on ET plus CDK4/6 inhibitors to a switch of ET plus ribociclib or ET plus placebo [3]. PFS was the primary endpoint of this study.
Patients who received ribociclib had a significantly longer median PFS than patients who received placebo (2.76 vs 5.29 months; HR 0.57; P=0.006). In addition, the 12-month PFS rate was approximately 3 times higher in the ribociclib arm (24.6% vs 7.4%). The results appeared to be consistent across subgroups, including the ‘prior fulvestrant/exemestane’ and ‘prior palbociclib/ribociclib’ subgroups.
ET plus ribociclib had a manageable safety profile. Neutropenia with a grade ≥3 was more common in patients on ribociclib (38% vs 0%) but only 2 patients experienced febrile neutropenia. Furthermore, 2 patients on ribociclib had pneumonitis (1 grade 3), and 3 patients experienced grade 3 infections, compared with 0 in the placebo group.
Interestingly, an exploratory analysis showed that patients with ESR1 wildtype mutational status may benefit more from additional ribociclib than patients with ESR1-mutated tumours (HR 0.30 vs HR 1.22). Prof. Kalinsky stressed that these were exploratory outcomes and should be interpreted as hypothesis-generating data only.
Prof. Claudine Isaacs (Georgetown University, Washington DC, USA) responded to these results with enthusiasm and caution. “This is the first well-designed, randomised trial to assess the applicability of CDK4/6 inhibitors and switch of ET after disease progression. However, the current study is too small to deliver practice-changing data in my opinion and it remains unclear whether we need to switch both ET and CDK4/6 inhibitors. Fortunately, other phase 2 and 3 trials are underway to investigate these issues.”
- Hortobagyi GN, et al. N Engl J Med. 2022;386:942–950.
- Wander SA, et al. J Natl Compr Canc Netw. 2021;1–8.
- Kalinsky K, et al. A randomized, phase II trial of fulvestrant or exemestane with or without ribociclib after progression on anti-estrogen therapy plus cyclin-dependent kinase 4/6 inhibition (CDK 4/6i) in patients (pts) with unresectable or hormone receptor-positive (HR+), HER2-negative metastatic breast cancer (MBC): MAINTAIN trial. LBA1004, ASCO 2022 Annual Meeting, 3‒7 June, Chicago, IL, USA.
Copyright ©2022 Medicom Medical Publishers
Posted on
Table of Contents: ASCO 2022
Featured articles
Breast Cancer
Sacituzumab govitecan meets primary endpoint
Shaky OS results of palbociclib in ER-positive/HER2-negative breast cancer
Practice-changing results of T-DXd in HER2-low breast cancer
SET2,3 to inform on chemotherapy decisions in ER-positive breast cancer
Metastasis-directed therapy fails in oligometastatic breast cancer
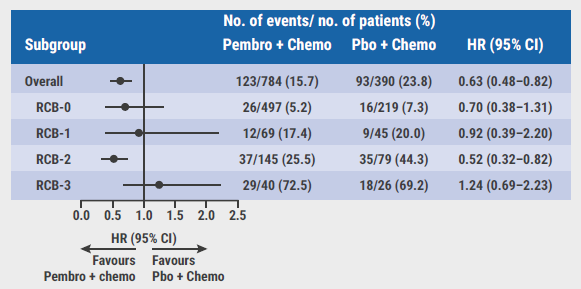
Analysis by residual cancer burden further clarifies effect of pembrolizumab
Contribution of metastatic therapies on mortality reduction in breast cancer
Radiotherapy may be omitted in breast cancer patients
Promising data for ribociclib after progression on ET plus CDK4/6 inhibitors in HR-positive/HER2-negative metastatic breast cancer
7-gene biosignature: Benefits of endocrine therapy and radiotherapy in breast cancer risk groups
Lung Cancer
Additional tiragolumab does not help patients with untreated small cell lung cancer
Success for serplulimab plus chemotherapy in small cell lung cancer
Adagrasib safe and clinically active in non-small cell lung cancer
Long-term benefits of combined immunotherapy over chemotherapy in non-small cell lung cancer
Effect of KRAS mutations and PD-L1 expression on therapy response in non-small cell lung cancer
Melanoma
First results on distant metastasis-free survival in stage II melanoma
Higher response rates for concurrent triple therapy versus sequential therapy in melanoma
Genitourinary Cancers
Exploratory treatment options fail in ccRCC
Adjuvant everolimus did not benefit high-risk renal cell carcinoma
Cabozantinib fails as first-line maintenance therapy in urothelial cancer
177Lu-PSMA-617 is a valid treatment option for PSMA-positive mCRPC
Enzalutamide performs well in metastatic hormone-sensitive prostate cancer
Haematologic Malignancies
Autologous stem cell transplantation plus RVd improves PFS in multiple myeloma
Novel first-line treatment option for mantle cell lymphoma
Promising results for novel CAR-T therapy in relapsed/refractory multiple myeloma
Gastrointestinal Cancers
Panitumumab beats bevacizumab in RAS wildtype left-sided metastatic colorectal cancer
Spectacular results for dostarlimab in mismatch repair deficient rectal cancer
Triplet chemotherapy beats doublet chemotherapy in colorectal cancer liver metastases
To resect or not to resect primary tumours in stage IV colon cancer?
Novel treatment option for KRAS wildtype pancreatic cancer
Gynaecological Cancers
Primary results of rucaparib in ovarian cancer
Trabectedin not superior to chemotherapy in recurrent epithelial ovarian cancer
Encouraging results of relacorilant in ovarian cancer
Miscellaneous Topics
Bacterial decolonisation effective against radiation dermatitis
New standard-of-care for cisplatin-ineligible locally advanced head and neck squamous cell carcinoma
Ifosfamide is likely to be the go-to therapy in recurrent Ewing sarcoma
Dabrafenib plus trametinib candidates for standard-of-care in BRAF V600-mutated paediatric low-grade glioma

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com