About 2 third of resuscitated OHCA patients without primarily obvious non-cardiac pathology do not present ST-elevation on the ECG [3]. Pros and cons of an instant coronary angiogram in these patients are still under debate [1,2]. The TOMAHAWK study (NCT02750462) hypothesised that the unselected immediate angiogram would be advantageous for OHCA patients compared with a delayed/selective angiogram. The trial randomised 554 patients over 30 years of age from various sites in Germany and Denmark who met the inclusion criteria of documented OHCA with return of spontaneous circulation (ROSC). ST-elevation in the ECG was among the reasons for exclusion. The primary endpoint was defined as all-cause mortality at 30 days.
The median age in the cohort was 70 years, roughly 38% had a prior diagnosis of coronary artery disease, and more than 50% presented a shockable first monitored rhythm. The timespan from OHCA to return ROSC was 15 min in both study groups. In the immediate group, 95.5% received an angiogram that was performed within 3 hours after OHCA, while 62.2% of the delayed group patients were taken to the Cath lab at a median of 46.9 hours after their arrest.
Overall, there was no significant difference between the arms in the primary endpoint (HR 1.28; 95% CI 1.00–1.63). “If you take the composite of all-cause mortality or severe neurological deficit, this actually becomes statistically significant, yet not accounted for multiple testing; so, this is just hypothesis generating,” Prof. Steffen Desch (University Heart Center Lübeck, Germany) highlighted one of the key secondary outcomes. Several relevant subgroups were also assessed without reaching statistical significance.
Although this has to be considered a neutral trial, discussant Prof. Susanna Price (Royal Brompton Hospital, UK) stressed that it answered an important question [4]. “It gives me information that is useful regarding the opportunity to minimise harm, which is a lot of what critical care is about. So, we do not necessarily have to move these patients very acutely when they just come into the ED. This has implications for resource utilisation, but it also has implications for mobilising patients around the hospital during COVID 19,” she underlined.
- Desch S. TOMAHAWK: Immediate angiography after out-of-hospital cardiac arrest. Hot Line Session, ESC Congress 2021, 27–30 August.
- Desch, S. N Engl J Med 2021;29 Aug. DOI:1056/NEJMoa2101909.
- Dumas F, et al. Circ Cardiovasc Interv. 2010;3(3):200-207.
- Price S. TOMAHAWK – Discussant review. Hot Line Session, ESC Congress 2021, 27–30 August.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: ESC 2021
Featured articles
2021 ESC Clinical Practice Guidelines
2021 ESC Guidelines on Heart Failure
2021 ESC/EACTS Guidelines on Valvular Heart Disease
2021 ESC Guidelines on Cardiac Pacing and Cardiac Resynchronisation Therapy
2021 ESC Guidelines on Cardiovascular Disease Prevention
Best of the Hotline Sessions
Empagliflozin: First drug with clear benefit in HFpEF patients
CardioMEMS: neutral outcome but possible benefit prior to COVID-19
Cardiac arrest without ST-elevation: instant angiogram does not improve mortality
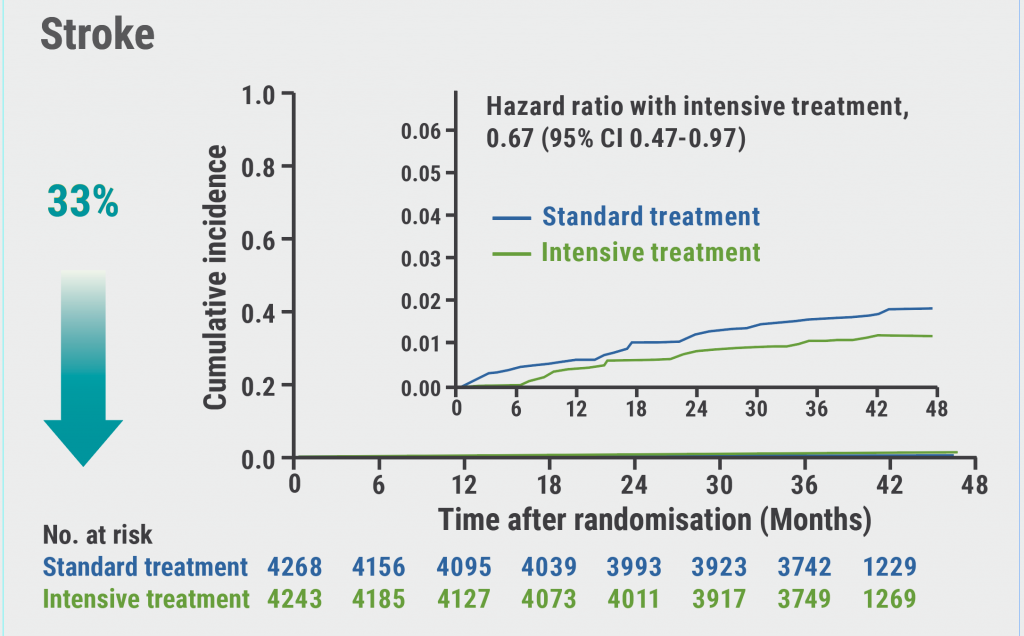
Older hypertensive patients benefit from intensive blood pressure control
Antagonising the mineralocorticoid receptor beneficial for patients with diabetes and CKD
Late-Breaking Science in Heart Failure
Valsartan seems to attenuate hypertrophic cardiomyopathy progression
Dapagliflozin reduces incidence of sudden death in HFrEF patients
Late-Breaking Science in Hypertension
Smartphone app improves BP control independent of age, sex, and BMI
QUARTET demonstrates that simplicity is key in BP control
Salt substitutes: a successful strategy to improve blood pressure
Late-Breaking Science in Prevention
NATURE-PCSK9: Vaccine-like strategy successful in lowering CV events
Polypill: A successful tool in primary prevention
Important Results in Special Populations
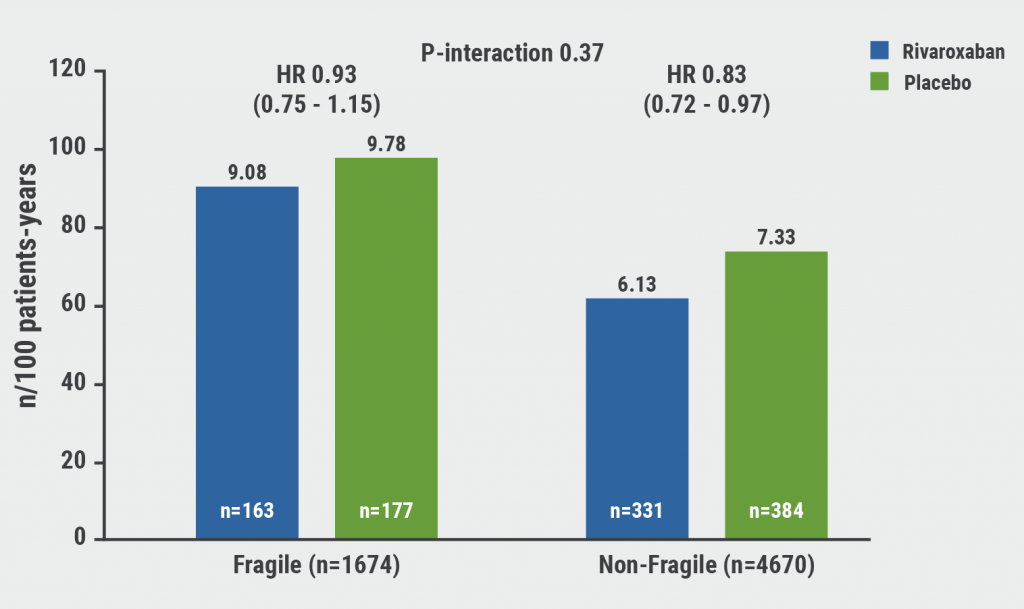
VOYAGER PAD: Fragile or diabetic patients also benefit from rivaroxaban
COVID-19 and the Heart
Rivaroxaban improves clinical outcomes in discharged COVID-19 patients
COVID-19: Thromboembolic risk reduction with therapeutic heparin dosing
Long COVID symptoms – Is ongoing cardiac damage the culprit?
ESC Spotlight of the Year 2021: Sudden Cardiac Death
Breathing problems: the most frequently reported symptom before cardiac arrest
Lay responders can improve survival in out-of-hospital cardiac arrest
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy