In patients with GCA, the use of the interleukin-6 receptor inhibitor tocilizumab in combination with 26-week prednisone tapering resulted in higher rates of sustained glucocorticoid-free remission compared with placebo and prednisone tapering in week 52 of the GiACTA trial [2]. Dr John Stone (Massachusetts General Hospital, Boston, USA) et al. aimed to investigate longer-term efficacy and safety of tocilizumab in GCA patients in this 2-year long-term extension of the GiACTA trial.
Patients in clinical remission (n=127) at the end of the double-blind period were asked to stop tocilizumab treatment. Of these, 51 patients (40%) maintained clinical remission during the extension study. The median time to first flare was longer for patients who were originally treated compared with those originally on placebo. The results further showed that disease flares tended to be resolved more quickly in those who originally received tocilizumab treatment. Rates of serious adverse events per were comparable for patients who never received tocilizumab and those who did (23.1 vs 25.4 per 100 patient-years), and rates of serious infections were 4.6 and 3.5 per 100 patient-years, respectively.
- Stone JH. et al. Abstract OP0140. EULAR 2019
- Stone JH, et al. N Engl JMed. 2017 Jul 27;377(4):317-328.
Posted on
Table of Contents: EULAR 2019
Featured articles
Efficacy and safety of ixekizumab versus adalimumab in patients with PsA
Rheumatoid Arthritis
Cohort study shows improvement during 25 years of RA treatment
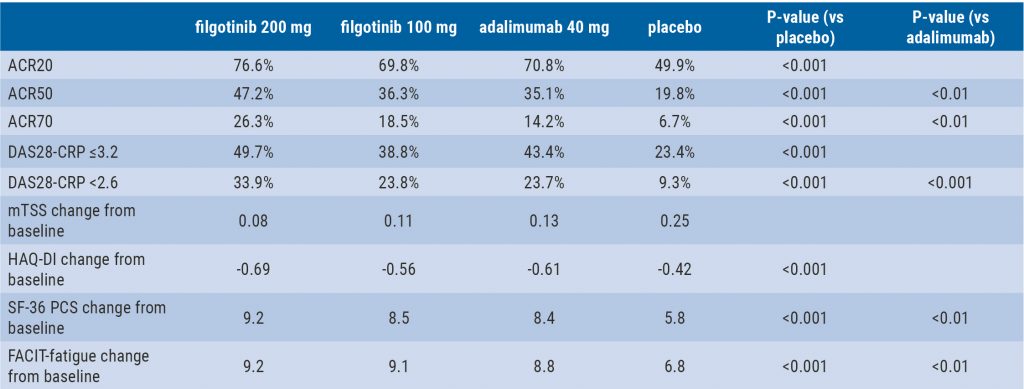
Filgotinib in RA patients with inadequate response or naïve to methotrexate
Clinical effectiveness of fenebrutinib in RA patients with methotrexate or TNFi failure
Short methotrexate stop is safe in patients with RA
Tofacitinib is safe according to real-world data analysis
Tapering of prednisone in RA patients who achieved low disease activity or remission with tocilizumab
Efficacy and safety of E6011 in RA patients with inadequate response to methotrexate
Preliminary efficacy and safety data of RG6125 in RA patients with an inadequate response to TNF inhibitors
Integrated 10-year analysis confirms safety profile abatacept
Switching among multiple infliximab biosimilars does not cause immunogenicity
Switch to sarilumab from adalimumab is efficacious and safe
Axial Spondyloarthritis
Treat-to-target approach emerging in axial spondyloarthritis
NSAIDs consumption is linked to patient-assessed disease activity and decreases with use of TNF inhibitors
Psoriatic Arthritis
Efficacy and safety of ixekizumab versus adalimumab in patients with PsA
Efficacy and safety of bimekizumab in patients with active PsA
Filgotinib is efficacious and safe in PsA
Ixekizumab improves signs and symptoms in TNFi-naïve PsA patients
Etanercept and methotrexate as first-line treatment in PsA
Unacceptable pain is common in patients with psoriatic arthritis
Osteoarthritis and Osteoporosis
Miscellaneous
Interstitial lung disease in rheumatic diseases and systemic sclerosis
Emapalumab in patients with macrophage activation syndrome
Support for tocilizumab use in giant cell arteritis
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com