
At the moment, endocrine therapy plus CDK4/6 inhibitor is the mainstay for the management of ER-positive/HER2-negative metastatic breast cancer. However, most patients eventually experience disease progression, including development of ESR1 mutations (mESR1). Elacestrant, an oral selective oestrogen receptor degrader (SERD), demonstrated preclinical and clinical activity in a phase 1 trial in ER-positive metastatic breast cancer, including responses in patients with prior fulvestrant, CDK4/6 inhibitor, and mESR1 tumours, thus forming the rationale for the phase 3 EMERALD trial (NCT03778931) [1].
EMERALD enrolled 477 postmenopausal patients (228 with mESR1) with ER-positive/HER2-negative metastatic breast cancer who had received 1–2 prior lines of endocrine therapy and ≤1 line of chemotherapy in the metastatic setting, and who had prior progression on endocrine therapy plus a CDK4/6 inhibitor. Patients were randomised 1:1 to elacestrant (400 mg orally daily) or standard of care (investigator’s choice of fulvestrant or an aromatase inhibitor). Dr Aditya Bardia (Massachusetts General Hospital, MA, USA) presented the results [2].
A 30% reduction in the risk of progression in the elacestrant arm in all patients was measured (HR=0.697; P=0.0018) and a 45% reduction in the risk of progression in patients with mESR1 (HR=0.546; P=0.0005; see Figure). Progression-free survival rate at 12 months was 22.3% with elacestrant versus 9.4% with standard of care in all patients and 26.8% versus 8.2% in the mESR1 subgroup. For both endpoints, results in key prespecified subgroups –including visceral metastases, number of prior lines of therapy, and pre-treatment with fulvestrant– were consistent with the overall outcome. The prespecified interim overall survival analysis planned at the time of the final progression-free survival analysis demonstrated a trend in favour of elacestrant in all patients and in patients with mERS1 (HR=0.751 and 0.592, respectively).
Figure: Probability of progression-free survival for elacestrant versus standard of care in patients with ESR1-mutatedtumours [2].
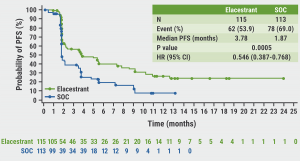
PFS, progression-free survival; SOC, standard of care.
“Elacestrant is the first oral selective oestrogen receptor degrader to demonstrate a statistically significant and clinically meaningful improvement of progression-free survival in patients with ER-positive/HER2-negative metastatic breast cancer in the second-line and third-line settings, including for patients whose tumours harbour ESR1 mutations,” said Dr Bardia.
- Bardia A, et al. J Clin Oncol 2021;39:1360–1370.
- Bardia A, et al. Elacestrant, an oral selective estrogen receptor degrader (SERD), vs investigator’s choice of endocrine monotherapy for ER+/HER2- advanced/metastatic breast cancer (mBC) following progression on prior endocrine and CDK4/6 inhibitor therapy: Results of EMERALD phase 3 trial. GS2-02, SABCS 2021 Virtual Meeting, 7–10 December.
Copyright ©2022 Medicom Medical Publishers
Posted on
Table of Contents: SABCS 2021
Featured articles
Early-Stage Breast Cancer
Aromatase inhibitors outperform tamoxifen in premenopausal women
Concurrent taxane plus anthracycline most beneficial in reducing risk of breast cancer
Reduced risk of recurrence with ovarian suppression plus tamoxifen/exemestane
Metformin does not improve outcomes in patients with early-stage breast cancer
Omitting sentinel lymph node biopsy improves arm symptoms
HR-positive/HER2-negative Breast Cancer
Addition of palbociclib to standard endocrine therapy does not improve outcome in adjuvant treatment
The SERD elacestrant improves outcomes for patients unresponsive to endocrine therapy
Consistent overall survival benefit of ribociclib in advanced breast cancer
Premenopausal women benefit from adjuvant chemotherapy next to endocrine therapy
Promising anti-tumour activity of the CDK7-inhibitor samuraciclib plus fulvestrant
ctDNA is prognostic and predictive for response to ribociclib plus letrozole
Early switch to fulvestrant plus palbociclib beneficial for patients with ESR1 mutation
Triple-Negative Breast Cancer
Single-cell spatial analysis can predict response to neoadjuvant immunotherapy
Neoadjuvant pembrolizumab plus chemotherapy benefits event-free survival in TNBC
Early use of ctDNA testing can identify likelihood of relapse in TNBC
Pembrolizumab plus chemotherapy benefits patients with combined positive score ≥10
Neratinib plus trastuzumab plus fulvestrant shows encouraging clinical activity
Phase 1–3 Trials
Datopotamab deruxtecan shows promising anti-tumour activity
Trastuzumab deruxtecan outperforms trastuzumab emtansine
Nivolumab plus ipilimumab serve promising dual checkpoint inhibition
Entinostat plus exemestane improves progression-free survival in Chinese patients
Efficacy of pyrotinib plus capecitabine confirmed in previously treated patients
Basic and Translational Research
Using genomics to match treatments improves outcomes
Loss of ASXL1 tumour suppressor promotes resistance to CDK4/6 inhibitors
Inducers of ferroptosis are potential drugs to target p53-mutated TNBC cells
MAPK-pathway alterations are associated with resistance to anti-HER2 therapy
Genomic signatures of DCIS define biology and correlate with clinical outcomes
BRCA2 linked to inferior outcomes with CDK4/6 inhibitors plus endocrine therapy
Miscellaneous
Olaparib is well tolerated as an additional treatment
Race effects the likelihood to develop lymphoedema following breast cancer treatment
Sentinel lymph node staging is non-inferior to complete axillary lymph node dissection
One in 7 breast cancers detected during screening are overdiagnosed
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com