
“Approximately half of RA patients lack treatment responses to expensive biologic therapies that also carry the risk of side effects. Predictive markers of response could help stratify RA,” said Prof. Costantino Pitzalis (Barts and The London School of Medicine and Dentistry, United Kingdom). “This leaves a major unmet and urgent clinical need to identify markers of treatment response to avoid delays in disease control, unnecessary exposure to potentially toxic drugs, and considerable waste of resources.” B cells are pivotal to RA pathogenesis, validated by the efficacy of the B cell-depleting agent rituximab, which is approved for use in RA patients after inadequate response to conventional synthetic DMARDs and TNF inhibitor. However, only 30% of these difficult-to-treat patients achieve an ACR50 response in disease activity at 6 months after starting rituximab.
More than half of patients with early RA have low B cell infiltration
An earlier study has shown that the presence of specific cellular/molecular synovial signatures exists in early RA and allows prediction of disease severity/progression and therapeutic response to treatment [2]. In this study, more than 50% of patients with early RA had low levels or an absence of B cell infiltration in their synovial tissue.
The rationale for the study presented at ACR [1], was that alternative B cell independent pathways drive inflammation in this subgroup of patients, and that alternative biologic agents to rituximab should work more effectively in these patients. This 48-week, phase 4, open-label, randomised controlled trial evaluated whether or not stratifying RA patients according to synovial B cell-rich or -poor status would help predict response to rituximab. Patients were recruited from 19 European medical centres and did not respond or were intolerant to conventional synthetic DMARD therapy and at least one TNF inhibitor. At the beginning of the trial, synovial tissue samples were histologically classified as either B cell-rich or B cell-poor to balance the randomisation of 164 patients in equal groups to receive either rituximab or tocilizumab. At 16 weeks, the researchers tested the superiority of tocilizumab over rituximab in the B cell-poor patient population. The study’s primary endpoint was a clinical disease activity index (CDAI) improvement of ≥50% from baseline. The co-primary endpoint was the Major Treatment Response, defined as a CDAI improvement of ≥50% along with a CDAI ≤10.1. The secondary outcomes included an assessment of CDAI response in the B cell-rich patient cohort, where the non-inferiority of rituximab compared with tocilizumab was evaluated. In addition, safety data for the therapies up to week 48 of the trial were collected.
Of the randomised patients, 81 of 83 who received rituximab and 73 of 81 who received tocilizumab completed treatment till week 16 of the trial. Baseline characteristics among the 2 treatment groups were similar. In the B cell-poor cohort, a numerically higher proportion of patients responded to tocilizumab (56.1%) compared with rituximab (44.7%), considering the primary outcome. A significantly greater proportion of patients achieved a Major Treatment Response with tocilizumab (46.3%) compared with rituximab (23.7%). Tocilizumab was also superior with regard to several additional secondary endpoints, e.g. the number of patients reaching moderate or good EULAR response and the proportion of patients in remission (36.6% with tocilizumab vs 15.8% with rituximab). In contrast, in the B cell-rich cohort no significant differences were shown in the majority of endpoints.
Patients treated with tocilizumab had a higher number of adverse and serious adverse events, such as infections, compared with those treated with rituximab. Overall, tocilizumab was clearly more effective than rituximab in the B cell-poor population who have failed conventional synthetic DMARDs and TNF inhibitor therapy. “These findings are important as they indicate that patients with low level of B cells in the synovial tissue are less likely to respond to rituximab and should be treated with alternative medications,” concluded Prof. Pitzalis. Serum autoantibody levels are well established predictors of response to rituximab so an integrated analysis of synovial B cell histology vis a vis serum autoantibody levels in predicting response is awaited.
- Pitzalis C et al. Abstract 2911. ACR 2019, 9-13 November, Atlanta (GA/USA).
- Humby F et al. Ann Rheum Dis 2019:78:761-72.
Posted on
Table of Contents: ACR 2019
Featured articles
Late-Breaking Abstracts
Lowest risk of infection after therapy with an IL-12/IL-23 blocker
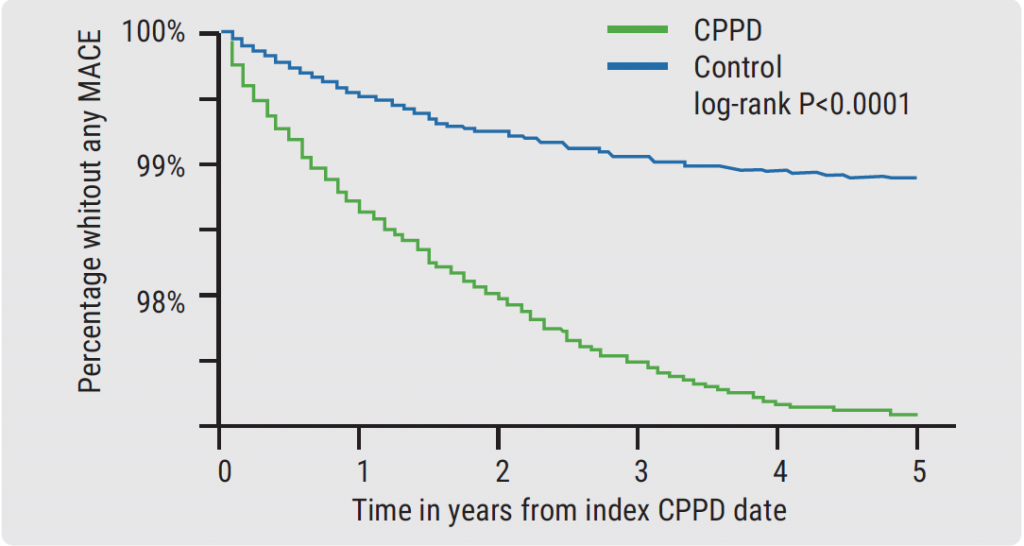
Calcium pyrophosphate deposition disease: an independent risk factor for cardiovascular complications
Proteome abnormalities improve prediction of RA development
RA patients in remission benefit from continued therapy with conventional DMARDs
Selective IL-23 blocker shows remarkable efficacy in patients with psoriatic arthritis
Corticosteroid therapy in GCA: higher platelets – lower relapse rate
Spotlight on Rheumatoid Arthritis
Filgotinib promising in RA patients naïve to methotrexate
Sustained efficacy of monotherapy with upadacitinib after 48 weeks
Biologics show similar activity in patients with elderly-onset RA
Tocilizumab outperforms rituximab in RA patients with low level of synovial B cell infiltration
Treatment decisions should not be guided by ultrasound findings
Cancer treatment with checkpoint inhibitors in RA patients?
What is Hot in Systemic Lupus Erythematosus
Anifrolumab succeeds in second phase 3 trial in SLE
Depression closely related to fatigue in SLE patients
Spondyloarthritis – The Beat Goes On
Psoriasis onset determines sequence of symptoms
Higher psychiatric comorbidity in women with PsA
JAK1 inhibition shows remarkable efficacy in AS
CARDAS study shows increased prevalence of cardiac valvular disorders in AS patients
Osteoarthritis – State-of-the-Art
Hand OA: low-dose corticosteroids improve symptoms
Opioids: no quality of life benefits for OA patients
Walking speed is a predictor of mortality in patients with knee OA
Reproductive Issues in Rheumatic Disease
Few serious infections in offspring with exposure to non-TNFi biologics or tofacitinib
Prevention of congenital heart block may be possible with hydroxychloroquine
TNFi for RA during pregnancy – to stop or not to stop?
Vasculitis – Novel Treatment Modalities
Rituximab maintenance superior to azathioprine in ANCA-associated vasculitis
Prolonged remission after stop of tocilizumab for patients with giant cell arteritis
Best of the Posters
Antifibrotic therapy slows disease progression independent of corticosteroid use
Fibromyalgia patients often experienced abuse in childhood
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com