
In the current EULAR guidelines, tapering of a biologic or small molecule is recommended in patients with RA in sustained remission while retaining the conventional (cs) disease-modifying antirheumatic drugs (DMARDs), usually methotrexate [2]. However, the knowledge about whether csDMARDs can be tapered in RA remission is limited. The primary objective of the non-inferiority ARCTIC REWIND trial was to assess the effect of tapering of csDMARDs on the risk of flares in RA patients in sustained clinical remission.
A total of 160 RA patients in clinical remission for at least 12 months on stable csDMARD therapy were randomly assigned to continued stable csDMARD or half dose csDMARD, with visits every 4 months. All patients were in Disease Activity Score (DAS) remission with no swollen joints (of 44 joints assessed). The primary endpoint was the proportion of patients with a disease flare during the 12-month study period (a combination of DAS >1.6, a change in DAS >0.6, and at least 2 swollen joints, or when both the physician and patient agreed that a clinically significant flare had occurred). Radiographic joint damage at 0 and 12 months was scored by van der Heijde modified Sharp score (progression: ≥1 unit change/year).
In the stable csDMARD arm, 6.4% of patients experienced a flare, compared with 24.7% in the half-dose arm. Superiority of the stable csDMARD therapy was also noticed in the methotrexate monotherapy users (78.2% of patients in the stable csDMARD arm and 84.4% in the half-dose csDMARD arm). In addition, the continued therapy with the full csDMARD dose showed advantages with regard to progression of radiographic joint damage: 79.5% of patients on stable dose showed no progression compared with 62.7% in the half-dose arm. After 1 year, 91.8% of patients in the stable arm and 85.1% in the half-dose arm were in DAS remission. Tolerability was comparable in 2 arms. The authors concluded that RA patients in remission benefit from a stable dose with csDMARDs, since it leads to significantly fewer disease activity flares and less frequent radiographic joint damage progression than tapered csDMARD treatment.
The results of ARCTIC REWIND are in line with the recently published TARA study where tapering a TNF inhibitor in RA patients in remission resulted in similar flare rates compared with tapering methotrexate. Thus, these authors also concluded that it is more sensible to taper the TNF inhibitor first due to possible cost reductions and fewer long-term side effects [3]. Therefore, the suggestion to taper biologics and small molecules in the 2016 guidelines of the ACR will get a level A recommendation in the updated guidelines.
- Lillegraven S, et al. Abstract L08. ACR 2019, 9-13 November, Atlanta (GA/USA).
- Smolen JS, et al. Ann Rheum Dis 2017;76:960-77.
- van Mulligen E, et al. Ann Rheum Dis 2019:78:764-53
Posted on
Table of Contents: ACR 2019
Featured articles
Late-Breaking Abstracts
Lowest risk of infection after therapy with an IL-12/IL-23 blocker
Calcium pyrophosphate deposition disease: an independent risk factor for cardiovascular complications
Proteome abnormalities improve prediction of RA development
RA patients in remission benefit from continued therapy with conventional DMARDs
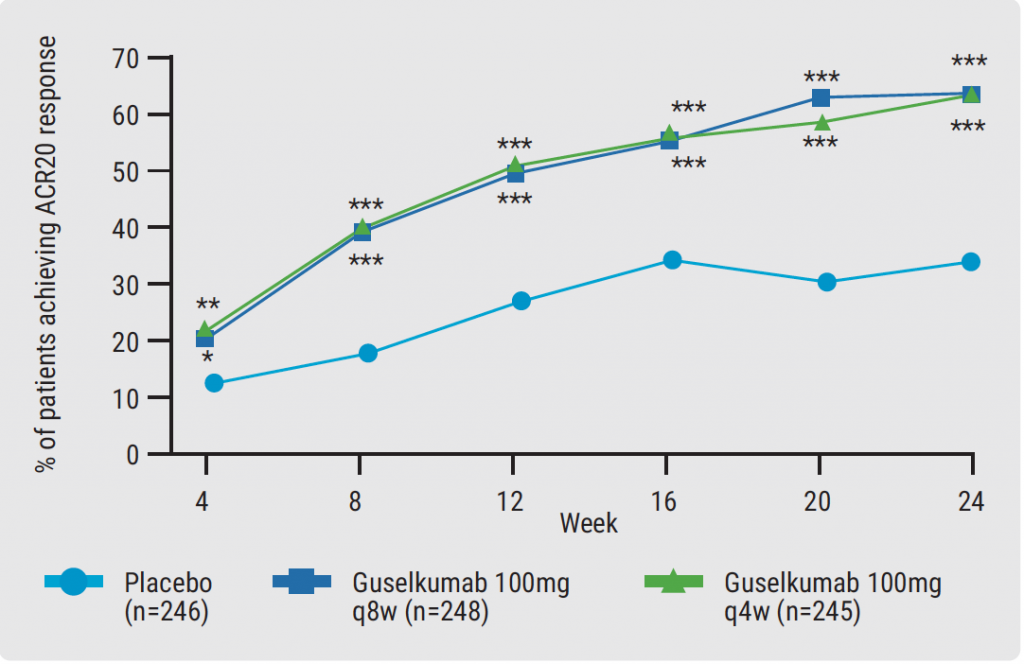
Selective IL-23 blocker shows remarkable efficacy in patients with psoriatic arthritis
Corticosteroid therapy in GCA: higher platelets – lower relapse rate
Spotlight on Rheumatoid Arthritis
Filgotinib promising in RA patients naïve to methotrexate
Sustained efficacy of monotherapy with upadacitinib after 48 weeks
Biologics show similar activity in patients with elderly-onset RA
Tocilizumab outperforms rituximab in RA patients with low level of synovial B cell infiltration
Treatment decisions should not be guided by ultrasound findings
Cancer treatment with checkpoint inhibitors in RA patients?
What is Hot in Systemic Lupus Erythematosus
Anifrolumab succeeds in second phase 3 trial in SLE
Depression closely related to fatigue in SLE patients
Spondyloarthritis – The Beat Goes On
Psoriasis onset determines sequence of symptoms
Higher psychiatric comorbidity in women with PsA
JAK1 inhibition shows remarkable efficacy in AS
CARDAS study shows increased prevalence of cardiac valvular disorders in AS patients
Osteoarthritis – State-of-the-Art
Hand OA: low-dose corticosteroids improve symptoms
Opioids: no quality of life benefits for OA patients
Walking speed is a predictor of mortality in patients with knee OA
Reproductive Issues in Rheumatic Disease
Few serious infections in offspring with exposure to non-TNFi biologics or tofacitinib
Prevention of congenital heart block may be possible with hydroxychloroquine
TNFi for RA during pregnancy – to stop or not to stop?
Vasculitis – Novel Treatment Modalities
Rituximab maintenance superior to azathioprine in ANCA-associated vasculitis
Prolonged remission after stop of tocilizumab for patients with giant cell arteritis
Best of the Posters
Antifibrotic therapy slows disease progression independent of corticosteroid use
Fibromyalgia patients often experienced abuse in childhood

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com