Data from a European cohort (Epi-IBD) of unselected IBD patients indicated a cost-saving effect of biological medications, despite their high acquisition costs [1]. Over a period of 5 years, overall direct healthcare expenses decreased in parallel with remarkably increasing expenditure on biologics, particularly in Crohn’s disease (CD) patients, and decreasing expenditure on standard medical treatments, surgery, and hospitalisation.
This is the first-ever prospective long-term analysis of healthcare costs in European IBD-patients in the era of biological treatments in Europe. Dr Johan Burisch (Frederiksberg Hospital, Denmark) received the Young ECCO (Y-ECCO) award for this abstract. The analysis was based on a population-based inception cohort of IBD patients from 31 centres in 20 European countries in 2010. Costs were specified for each centre. Of the 1,362 included IBD patients, 52% had UC, 37% CD, and 11% unclassified IBD.
Mean total expenditure per patient-year (PY) was highest in the first year in both Western and Eastern Europe, and then decreased. For CD patients, mean total expenditure was €5,579 in Y1 and €1,669 in Y5. For UC patients, it amounted to €3,612 and €674, respectively (see also Tables 1 and 2). The proportion spent on biologicals was lowest in the first year (11% and 2%, respectively) and rose to 55% and 25% in Y5. Expenditure on biological therapy increased in both Western Europe (PY1 €338, PY5 €516) and Eastern Europe (PY1 €31, PY5 €292). In both regions, this was paralleled by a steady decrease of costs of non-biological treatment, hospitalisation, and surgery. In a regression analysis, patients with worse disease phenotype as well as age ≥40 years generated higher costs. The overall outlay on biological therapy, expressed as a percentage of total expenditure, varied by age group: ≥40 years, 29%; 41-60 years, 21%; and ≥61 years, 11%. Dr Burisch added that expenditure on biologicals varied greatly per country, due to factors such as pricing and reimbursement.
Table 1: Mean total expenditure (€/patient) as well as proportion of expenditure spent on different categories of direct costs in patients with Crohn's disease [1]
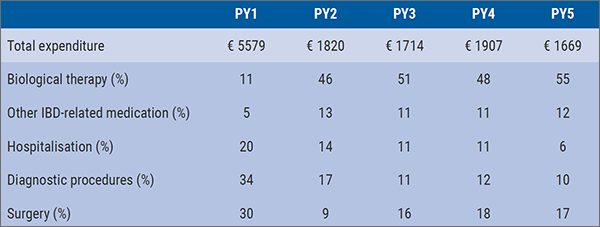
IBD, inflammatory bowel disease; PY, patient year
Table 2: Mean total expenditure (€/patient) as well as proportion of expenditure spent on different categories of direct costs in patients with ulcerative colitis [1]
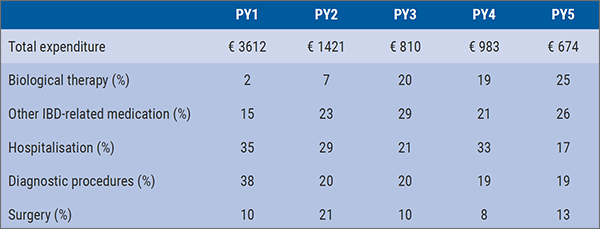
IBD, inflammatory bowel disease; PY, patient year
In a prospective Danish population-based cohort, the combined direct and indirect cost of IBD were assessed over a period of 10 years [2]. Direct costs for IBD remained high, but indirect costs did not surpass those of the control population. Total costs were mainly driven by hospitalisation; yet, over time, indirect costs accounted for a higher percentage, although they also decreased over the years. All incident patients (n=513) diagnosed between 2003 and 2004 in a well-defined area with CD (n=213) or UC (n=300) were followed prospectively until 2015. Direct and indirect costs were compared with a control population matched by age, sex, and municipality.
No significant differences were found in indirect costs between CD, UC, and the control population regarding paid sick leave, unemployment benefits, or loss of tax income. For CD patients, all direct costs (except for 5-ASA) were significantly higher than for UC patients. No differences were observed in diagnostic expenses (see Figure 1 for the distribution of expenses). Subgroup analyses only revealed significant increased direct expenses over time in patients with extensive colitis (proctitis: €2,273, left-sided: €3,606, extensive: €4,093, P<0.001). No variables were significantly associated with increased total costs in CD or UC patients.
Figure 1: Distribution of costs per year in patients with inflammatory bowel disease [2]
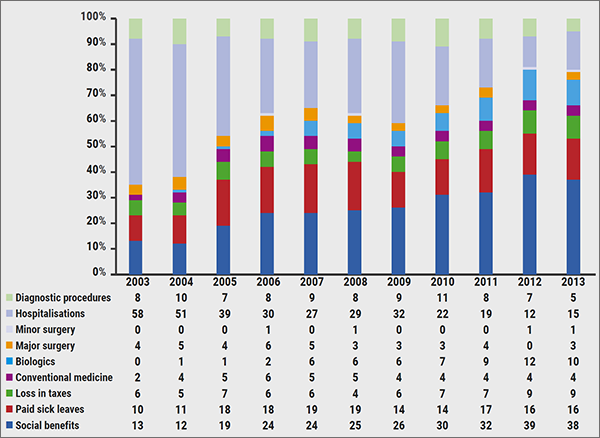
Conventional medicine: 5-aminosalicylic acid, topical steroids, corticosteroids, and immunosuppressants.
1. Burisch J, et al. ECCO 2019, OP015.
2. Lo B, et al. ECCO 2019, DOP82.
Posted on
Table of Contents: ECCO 2019
Featured articles
Interview with Prof. Janneke van der Woude
New Compounds: Study Results
Short-term and Long-term Treatment Results
The right drug for the right patient
Vedolizumab superior to adalimumab in ulcerative colitis
Complementary and Alternative Medicine
Crohn’s disease exclusion diet + partial enteral nutrition in paediatric Crohn’s disease
Microbial composition and psychological wellbeing
Remission
Early remission of Crohn’s disease prevents progression
Proactive adalimumab trough measurements
Observational Studies
IBD risk of treatment with IL-17 antagonists
Basic and Preclinical Research
Immune cells and microbes: a happy marriage?
Genetics
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy