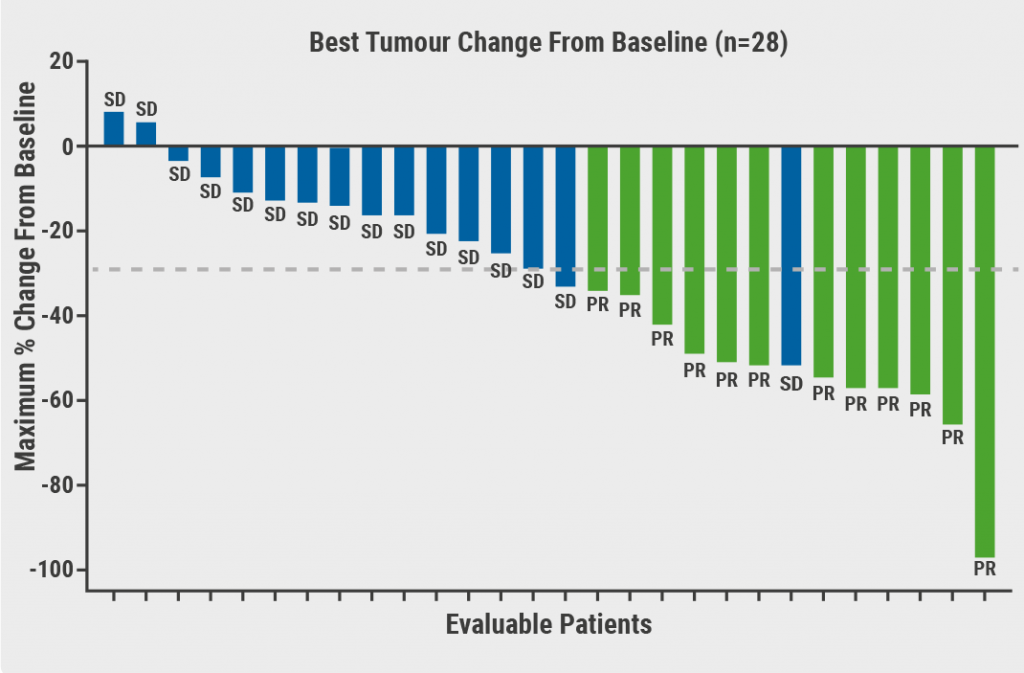
TKI therapy is an important backbone in the management of locally advanced or metastatic RCC, with significant survival advantage. However, TKI therapy is associated with significant toxicities which often lead to dose reduction and/or discontinuation of treatment. In addition, TKI therapy comes with high costs. The multicentre, randomised, phase 2/3 STAR trial (EudraCT 2011-001098-16) was designed to determine if a TKI drug-free interval strategy (DFIS) was non-inferior to a conventional continuation strategy (CCS) in the first-line treatment of advanced RCC. Outcomes were overall survival (OS) and Quality Adjusted Life Years (QALYs). Both co-primary endpoints (OS and QALYs) had to demonstrate pre-defined non-inferiority (≤7.5% for OS; ≤10% for QALYs) in intention-to-treat and per-protocol analyses for non-inferiority to be concluded. Prof. Janet Brown (University of Sheffield, UK) presented the first results of the STAR trial [1].
A total of 920 patients with newly diagnosed metastatic RCC who started treatment with sunitinib or pazopanib were 1:1 randomised to DFIS or CCS. Overall, 488 (53.0%) patients (CCS, n=240; DFIS, n=248) continued on trial post-week 24. Intention-to-treat and per-protocol analyses included 461 versus 458 patients and 453 versus 418 patients, respectively.
After 24 weeks of treatment, DFIS patients took a treatment break until disease progression, with additional breaks dependent on disease response and patient/clinician choice. Trial strategy continued until intolerance, progression on treatment, or death. At least one treatment break was mandated, with a median treatment break length of 87 days; 27% of patients had 3 or more treatment breaks.
For OS, in the intention-to-treat population, HR was 0.97 (95% CI 0.83–1.12), whereas in the per-protocol population, HR was 0.94 (95% CI 0.80–1.09). With a non-inferiority margin of 95% CI ≥0.812, this meant DFIS in the per-protocol population could not be regarded as non-inferior to CCS. However, consistent non-inferiority in both populations was demonstrated for QALYs. At 2 years, DFIS was associated with cost savings (£6,954 per-participant).
“Although OS just fell short of predefined non-inferiority, probably due to fewer than expected events, non-inferiority of DFIS for QALYs was demonstrated. DFIS also appeared to be highly cost-effective compared to CCS. In addition, DFIS was seen to be acceptable to patients and clinicians,” summarised Prof. Brown.
- Brown JE, et al. STAR: A randomised multi-stage phase II/III trial of standard first-line therapy (sunitinib or pazopanib) comparing temporary cessation with allowing continuation, in the treatment of locally advanced and/or metastatic renal Cancer (RCC). Abstract LBA28, ESMO Congress 2021, 16–21 September.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: ESMO 2021
Featured articles
Breast Cancer
Trastuzumab deruxtecan triples PFS
Novel conjugate meets primary endpoint
Longest survival benefit from first-line CDK4/6 inhibitor
Meta-analysis shows 6-months adjuvant trastuzumab is optimal
Double-positive results for triple-negative metastatic breast cancer
Survival after neoadjuvant therapy with trastuzumab-lapatinib plus chemotherapy
Postmenopausal breast cancer: extended letrozole reduces recurrence
Asian women also benefit from palbociclib plus letrozole
No PEARLs of survival with palbociclib plus endocrine therapy compared with capecitabine, but QoL better
Gastrointestinal Cancer
Neoadjuvant chemotherapy potential alternative to neoadjuvant chemoradiotherapy in LARC
Immune chemo-sensitisation looks promising in microsatellite-stable mCRC
Adagrasib shows promising clinical activity in heavily pretreated KRAS-mutated CRC
Automated detection of microsatellite status on unstained samples in early colon cancer
Consistent benefit of anti-PD-1 therapy for oesophageal and gastric cancer
HIPEC in gastric cancer with peritoneal metastases
ctDNA highly predictive in HER2-positive, advanced gastric or gastro-oesophageal junction cancer
Lung Cancer
Robust anticancer activity of trastuzumab deruxtecan in HER2-mutated NSCLC
Nivolumab/ipilimumab continues to provide survival benefit in unresectable MPM
Adjuvant atezolizumab lowers relapse rate in resected NSCLC
Three-year OS follow-up from CASPIAN trial
TCR clonality predicts pembrolizumab response in NSCLC
Melanoma
Adjuvant immunotherapy reduces risk of disease recurrence in stage II melanoma
IFN-γ signature predicts response to immunotherapy
Updated results of SECOMBIT trial
Combining T-VEC and pembrolizumab does not significantly improve survival in advanced, unresectable melanoma
Durable intracranial responses with nivolumab/ipilimumab
Genitourinary Cancer
TKI drug-free interval strategy not detrimental to conventional continuation strategy in RCC
Modified ipilimumab schedule reduces risk of grade 3/4 adverse events
Optimal neoadjuvant dose ipilimumab/nivolumab in stage III urothelial cancer
Better survival with neoadjuvant dose-dense MVAC regimen in MIBC
PARP inhibitor rechallenge improves PFS in ovarian cancer
Pembrolizumab prolongs survival in persistent, recurrent, or metastatic cervical cancer
Pembrolizumab has durable effect in previously treated MSI-H/dMMR advanced endometrial cancer
HRR mutational status is prognostic and predictive biomarker olaparib activity
Haematological Cancer
Mutational analyses are predictive in malignant lymphomas
Low numbers of M2 macrophages in tumour microenvironment associated with superior response to immunotherapy in Hodgkin lymphoma
COVID-19
Adequate response to SARS-CoV-2 vaccine in cancer patients
Cancer patients more likely to die from COVID-19 when hospital admittance is required
Third global survey of the ESMO Resilience Task Force
High COVID-19 mortality in Swiss cancer patients
Basic Science & Translational Research
Neutrophils negatively correlate with response to anti-PD-1 monotherapy in dMMR tumours
Tetraspecific ANKETs harnesses innate immunity in cancer therapies
Early ctDNA reduction in metastatic uveal melanoma correlates better with OS than RECIST response
Gut microbiota as a potential predictive biomarker

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy