
“Strategies that avoid a high proportion of first CV events are critical to reducing global CV disease (CVD) burden,” said Prof. Philip Joseph (McMaster University, Canada) [1]. Fixed-dose combination (FDC) treatment could substantially reduce CV risk, but more data is needed to quantify its efficacy. The so-called polypill in a single formulation usually contains 2+ blood pressure-lowering agents, a statin, and in some cases, aspirin. In a meta-analysis of long-term, randomised controlled trials (each including >1,000 participants >2 years follow-up), Prof. Joseph and his colleagues tested different FDC strategies versus controls for primary prevention. The primary objective was the prevention of a composite of CV death, MI, stroke, or revascularisation. In addition, the impact on individual CV outcomes and the difference between regimens with and without aspirin was evaluated.
Data from 3 large RCTs of FDC in primary prevention was included in the analysis: the TIPS-3 trial (NCT01646437), the HOPE-3 trial (NCT00468923), and the Polylran trial (NCT01271985) [3-5]. With 18,162 participants in these trials, this meta-analysis is the largest study to date showing the effect of polypill therapy in CVD prevention.
“There was a large difference in the primary outcome: with FDC, we saw a 38% reduction [versus control]. This became apparent within 1 year of follow-up and the curves continued to diverge,” Prof. Joseph said (see Figure). Likewise, single events were markedly reduced with a reduction of MI by 48%, a reduction of stroke by 42%, and a reduction of CV death by 35%. The polypill led to marked changes in risk factors: after a follow-up time of 2.1 years, LDL concentrations in the FDC group were 22.6 mg/dl (0.58 mmol/L) lower than in the control group. After this time, systolic blood pressure showed a mean difference of 4.7 mmHg in favour of the polypill.
Figure: The primary endpoint of CV death, MI, stroke, or revascularisation [1]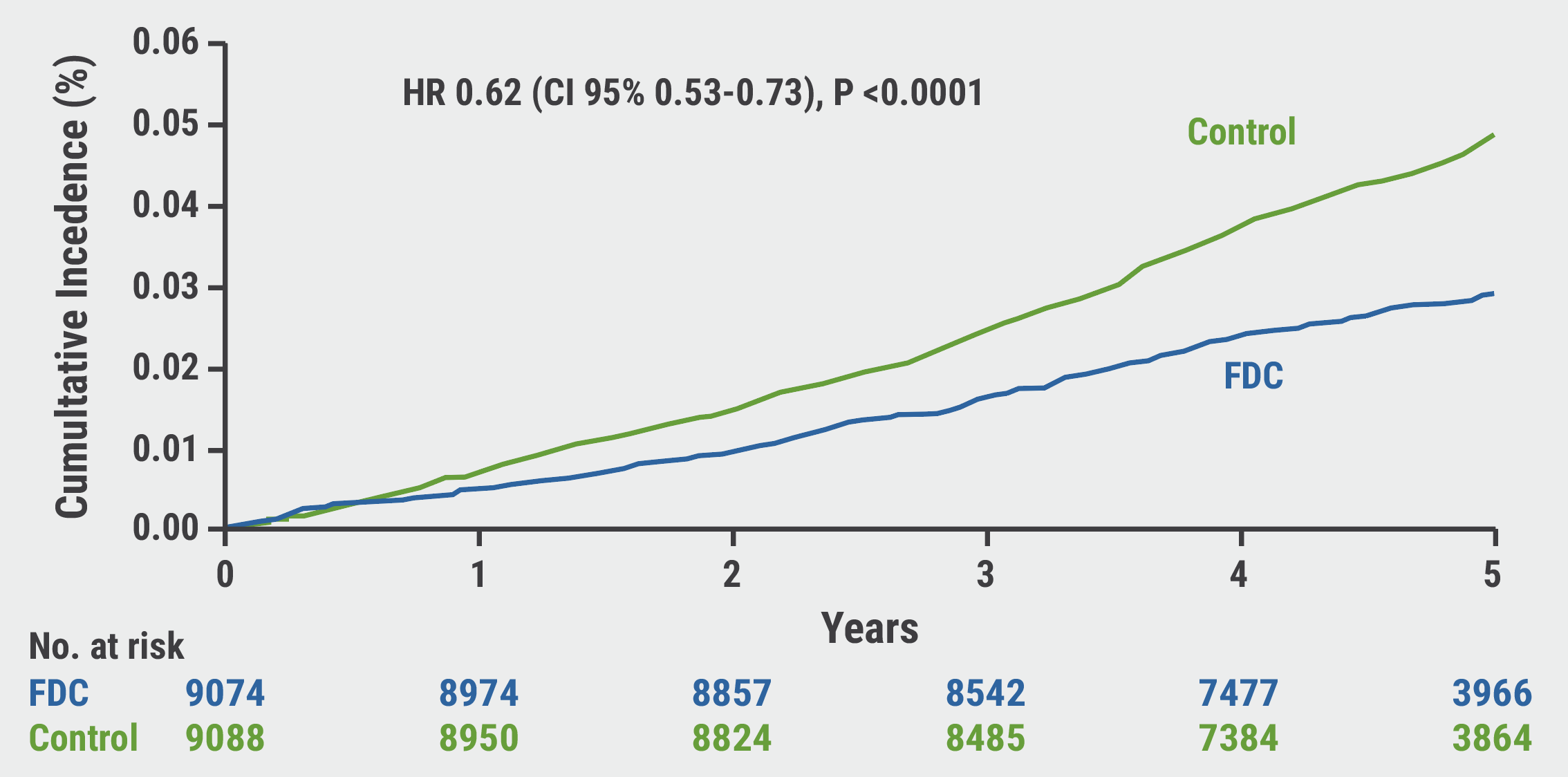 CI, confidence interval; FDC, fixed-dose combination; HR, hazard ratio.
CI, confidence interval; FDC, fixed-dose combination; HR, hazard ratio.
“The largest effects were seen in combinations that included aspirin, but the others were still very important,” Prof. Joseph said. Aspirin-containing regimens led to a reduction of CVD by 47%, a reduction of MI by 53%, and stroke by 51%. A subgroup analysis revealed that the benefit of FDC was most prevalent in the elderly (>66 years).
The analysis found no significantly elevated risk of haemorrhagic stroke or fatal bleeding, but a numerically increased risk of gastrointestinal bleedings was seen that failed to achieve statistical significance. Only 37 participants had to be treated with an aspirin-containing regimen to prevent 1 event of the primary outcome; in the total group, the number needed to treat was 51. Thus, Prof. Joseph advocated FDC treatment as a key strategy in primary CVD prevention.
- Joseph P. Fixed-dose combination therapies with and without aspirin in primary CVD prevention. Late-breaking trials in prevention, ESC Congress 2021, 27–30 August.
- Joseph P, et al. Lancet 2021;Aug 29. DOI:10.1016/S0140-6736(21)01827-4.
- Yusuf S, et al. N Engl J Med 2021;384:216–228.
- Yusuf S, et al. N Engl J Med 2016;374:2021–2031.
- Roshandel G, et al. Lancet 2019;394:P672–83.
Copyright ©2021 Medicom Medical Publishers
Posted on

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com