
HFrEF
The 3 fundamental therapies for patients with HF with reduced ejection fraction (HFrEF) are angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), mineralocorticoid receptor antagonists (MRAs), and β-blockers. The first choice of therapy depends on heart rate, blood pressure, and renal function. “For example, in patients with an increased heart rate, β-blockers would be the first therapy of choice. If we want to expand from our fundamental therapies, angiotensin receptor-neprilysin inhibitor (ARNIs) and sodium-glucose co-transporter 2 (SGLT2) inhibitors are the available options. Although ARNIs provide a clear additional benefit for our patients, we have to consider blood pressure and tolerance of ACE inhibitors or ARBs.” An analysis of the PARADIGM-HF trial (NCT01035255) showed that patients on the ARNI sacubitril/valsartan with a baseline systolic blood pressure ≤110 mmHg experienced hypotensive events in 25% of the cases [2]. “Therefore, patients with a blood pressure <100 mmHg, in general, do not qualify for this expansion option.” On the other hand, SGLT2 inhibitors do not display much blood pressure lowering [3]. In addition, SGLT2 inhibitors may have an added benefit for renal function. Since half of the patients with HF have chronic kidney disease and the mortality in patients with HF increases when renal function drops (RR of 1.4 when eGFR <60), this is an important factor to consider [4,5]. “In summary, SGLT2 inhibitors might be favoured over ARNIs in less robust patients with HFrEF.”
HFpEF
“In patients with a preserved EF (HFpEF), there is no recommended routine neurohormonal therapy,” Prof. Stevenson continued. “Controversial indications for ARBs and MRAs, β-blockers for arrhythmias or ischaemia, and perhaps SGLT2 inhibitors for renal preservation are the options we currently have. In addition, although SGLT2 inhibitors show benefits in patients with HFpEF, the benefits may be limited to the lower EFs within this population [6].”
Obesity
“Importantly, we need to tackle obesity as a cause and aggravator of the disease. The prevalence of obesity is >30% in most [US] states. If we do not address this problem, the treatment effect of emerging therapies will remain limited. Semaglutide, a GLP-1 antagonist, showed a remarkable 18% weight reduction in overweight or obese adults in 2 recent studies. However, the tolerance of this agent is problematic in many patients [7,8].
In conclusion, therapy design in patients with HF and diabetes is challenging. The robustness, disease stage, and resources of the patients are important decision criteria, and the therapy effectiveness will remain limited in this population if obesity is not adequately addressed.
- Stevenson LW. An Abundance of Therapeutics: An Integrated Approach to Managing HF with DM. PR.ME.461, AHA 2021 Scientific Sessions, 13–15 November.
- Böhm M, et al. Eur Heart J. 2017;38(15):1132–1143.
- Böhm M, et al. J Am Coll Cardiol. 2021;78(13):1337–1348.
- Dries DL, et al. J Am Coll Cardiol. 2000;35(3):681–689.
- McGuire DK, et al. J Am Coll Cardiol. 2021;6(2):148–158.
- Packer M, et al. Circulation. 2021;144:1193–1195.
- Wilding JHP, et al. N Engl J Med 2021;384:989–1002.
- Rubino D, et al. J Am Coll Cardiol. 2021;325(14):1414–1425.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: AHA 2021
Featured articles
The scope of remote healthcare in hypertension and hyperlipidaemia
Atrial Fibrillation
New developments in remote diagnostics and monitoring of AF
Head-to-head: Efficacy of dabigatran versus warfarin on cognitive impairment
Posterior left pericardiotomy safe and effective in reducing atrial fibrillation
LAA ligation did not reduce recurrent atrial arrhythmias in persistent AF
Equal benefits of early rhythm control in AF subtypes
CVD Risk Reduction
Remote healthcare programme improves hypertension and lipid control
Novel oral PCSK9 inhibitor shows promising results for hypercholesterolaemia
REVERSE-IT: Interim analysis shows promising effect of bentracimab on ticagrelor reversal
No significant effect of aspirin on reducing cognitive impairment
Milvexian phase 2 data supports safety and efficacy for VTE prevention after total knee replacement
Network meta-analysis observes no clear effect of eicosapentaenoic acid on CV outcomes
Heart Failure
Empagliflozin efficacious in HF patients with preserved ejection fractions ≥50%
EMPULSE: Empagliflozin improves outcomes of acute heart failure
CHIEF-HF: Canagliflozin improves health status in heart failure
DREAM-HF: MPC therapy for HFrEF did not meet primary endpoint
Therapeutic approaches in heart failure with diabetes
Acute Coronary Syndrome
Ticagrelor cessation: early CABG non-inferior to delayed surgery
Distinguishing patients before AMI based on plaque morphology
Vascular Diseases: PVD
Rivaroxaban regimen beneficial after revascularisation for claudication
LIBERTY 360 shows quality-of-life improvements after peripheral vascular intervention
Deficient treatment outcomes after PVI in Black and low-income adults with PAD
REDUCE-IT: Cardiovascular risk reduction with icosapent ethyl in PAD
Vascular Diseases: CAD
Long-term reduced risk of CV events with ticagrelor plus aspirin after CABG
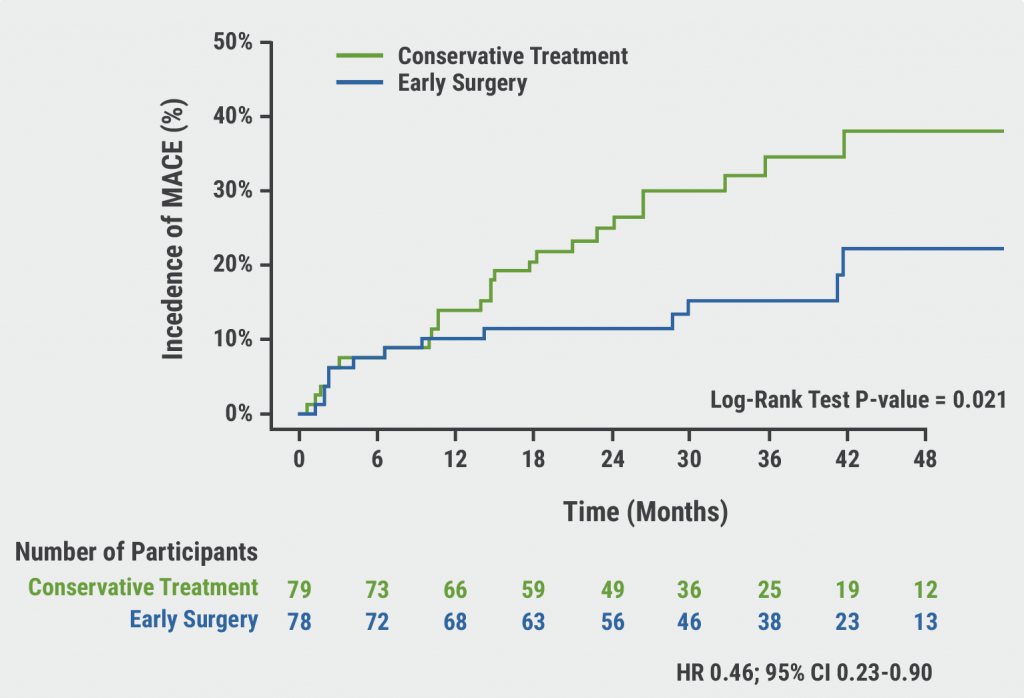
Early surgery outperforms conservative management in asymptomatic severe aortic stenosis
External support device for SVG grafts in CABG surgery shows promise
COVID-19 & the Heart
Blood pressure control disrupted during the pandemic
Icosapent ethyl did not reduce the risk of hospitalisation in COVID-19
Neutral effect of P2Y12 inhibitors in non-critical COVID-19 hospitalisations
COVID-19 mRNA vaccination benefits outweigh the risk for myocarditis
Other
2021 Guideline for Chest Pain: Top 10 takeaways
Accurate ejection fraction assessment in paediatric patients via artificial intelligence
Concomitant tricuspid annuloplasty reduces treatment failure in moderate tricuspid regurgitation

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com