
https://doi.org/10.55788/e8d7604b
TRILUMINATE (NCT03904147) was designed to evaluate the safety and effectiveness of medical therapy alone or percutaneous TEER the TriClipTM G4 Delivery System for severe TR usage [1]. First author Dr Paul Sorajja (Minneapolis Heart Institute, MI, USA) said over 450 participants had thus far been enrolled at 65 centres in the USA, Canada, and Europe; he went on to present the main results of the first 350 patients [2]. Key inclusion and exclusion criteria are shown in the Table.
Table: Enrolment criteria of the TRILUMINATE trial. Derived from [2]
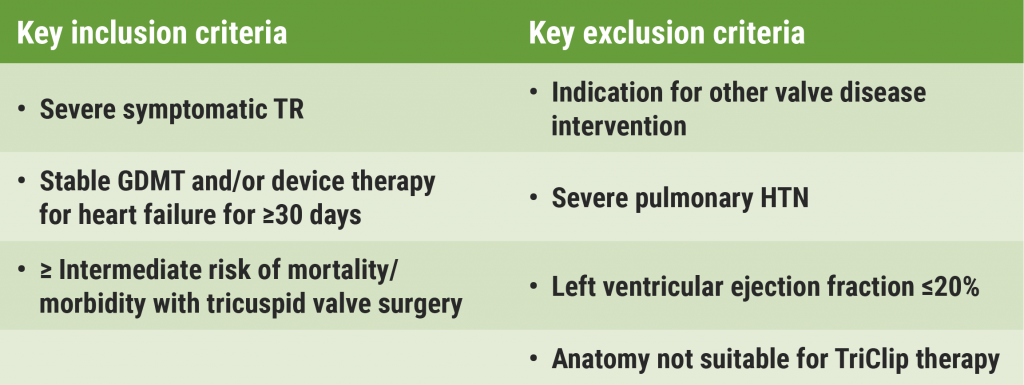
GDMT, guideline-directed medical therapy; HTN, hypertension.
The participants were randomly assigned to TEER (n=175) or medical therapy (n=175). The mean age was 78 years, and 54.9% were women. The primary endpoint was a composite assessed hierarchically of all-cause death or the number of participants with tricuspid valve surgery, hospitalisation for HF, and quality of life improvement assessed by the Kansas City Cardiomyopathy Questionnaire (KCCQ) at 1 year. The secondary endpoints were: 1) freedom from major adverse events (MAE) after procedure attempt at 30 days (in the experimental group only); 2) change in quality of life as measured with the KCCQ; 3) TR reduction to moderate or less at 30 days; 4) change in 6-minute walking distance (6MWD) at 1 year.
The results for the primary endpoint favoured the TEER group (win ratio 1.48; 95% CI 1.06–2.13; P=0.02). Dr Sorajja noted that this result was driven mainly by the improvement in quality of life. The incidence of death or tricuspid-valve surgery and hospitalisation for heart failure in both groups were similar. The KCCQ score improved by a mean (±SD) of 12.3±1.8 points, as compared with 0.6±1.8 points in the control group (P<0.001). TR was reduced by TEER to moderate or less in 87% of patients compared with only 4.8% in the control group; this reduction was sustained for 1 year of follow-up. The degree of TR reduction was related to the degree of improvement in quality of life. The 30-day MAE rate was only 1.7%; death and pacemaker implant both occurred in 0.6%. Survival without valve surgery was high at 1 year in both groups: around 90%.
“These results are very meaningful for a highly symptomatic population whose quality of life is impacted by TR,” said Dr Sorajja. “With the excellent benefit-to-risk ratio of the TriClip system, a historically untreated population will have a treatment option to improve their quality of life.”
- Sorajja P, et al. N Engl J Med 2023; Mar 4. DOI: 10.1056/NEJMoa2300525.
- Sorajja P, et al. Triluminate pivotal: A landmark randomized clinical trial of transcatheter tricuspid valve edge-to-edge repair for tricuspid regurgitation. Session 402-08, ACC Scientific Session 2023, 4–6 March, New Orleans, USA.
Copyright ©2023 Medicom Medical Publishers
Posted on
Table of Contents: ACC 2023
Featured articles
Pulmonary Arterial Hypertension
Sotatercept improves exercise capacity in patients with PAH
Fixed-dose macitentan plus tadalafil superior to either agent alone in PAH
Coronary Revascularisation
Immediate complete revascularisation non-inferior to staged complete revascularisation
RENOVATE-COMPLEX-PCI results support intravascular-guided PCI for complex lesions
Heart Failure and Cardiomyopathy
No need to restrict vigorous exercise in selected HCM patients?
No difference in CV outcomes between PET or CMR and SPECT
Interventional and Structural Cardiology
Benefits of MitraClip sustained to 5 years in COAPT trial
Transcatheter repair for patients with tricuspid regurgitation
Minimally invasive versus conventional sternotomy for mitral valve repair
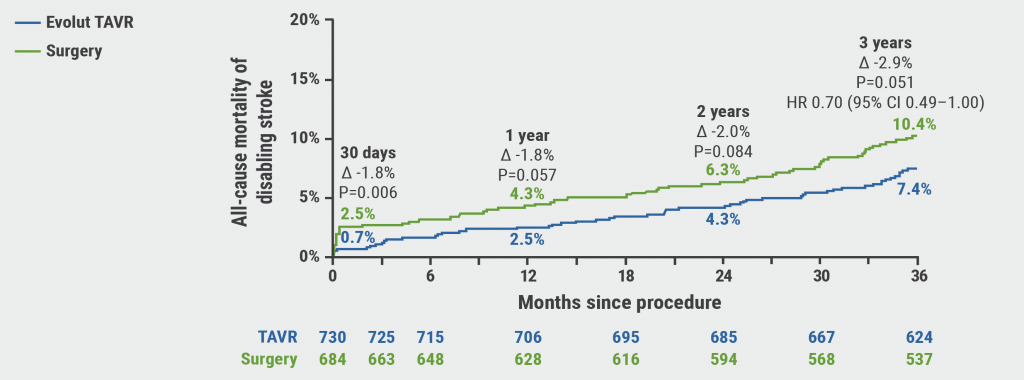
Durable benefits of TAVR versus surgical aortic valve replacement in aortic stenosis patients
PCI not better than GDMT in severe ischaemic cardiomyopathy
Prevention
Anticoagulation in non-critically ill hospitalised COVID patients
Statins associated with reduced heart dysfunction from anthracyclines
Multifaceted strategy improves prescription of therapies for diabetes and ASCVD
Dyslipidaemia
Bempedoic acid benefits statin-intolerant patients at high cardiovascular risk
Evolocumab improves coronary plaque morphology in stable CAD
Inflammation stronger predictor of MACE than cholesterol levels
Oral PCSK9 inhibitor significantly lowers LDL-C
Miscellaneous
Baxdrostat in patients with uncontrolled hypertension
Hormone therapy for gender dysphoria associated with increased CV risk
Pulsed-field ablation appears safe and effective for atrial fibrillation
Key correlates of incident dementia identified in the MESA study
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com