https://doi.org/10.55788/08fb868c
TAVR has been FDA-approved for patients with aortic stenosis of all surgical risk levels since 2019 and has now surpassed surgical AVR (SAVR) in procedural volumes in the USA, said Prof. John Forrest (Yale Medicine, CT, USA) [1]. The 2-year outcomes of the randomised, multicentre Evolut Low Risk trial (NCT02701283) showed that TAVR for the treatment of severe symptomatic aortic stenosis in low-risk patients was non-inferior to surgery for the primary endpoint of all-cause death or disabling stroke [2]. Prof. Forrest presented the 3-year clinical and echocardiographic outcomes from the Evolut Low Risk trial.
The participants of the Evolut Low Risk trial had severe aortic stenosis with a low risk of death from surgery (>3%). Patients with bicuspid aortic valves were excluded. Between 2016 and 2019, 1,414 patients were randomised to TAVR with a self-expanding, supra-annular valve (n=730) or surgery (n=684). The participants had a mean age of 74 years and 35% were women.
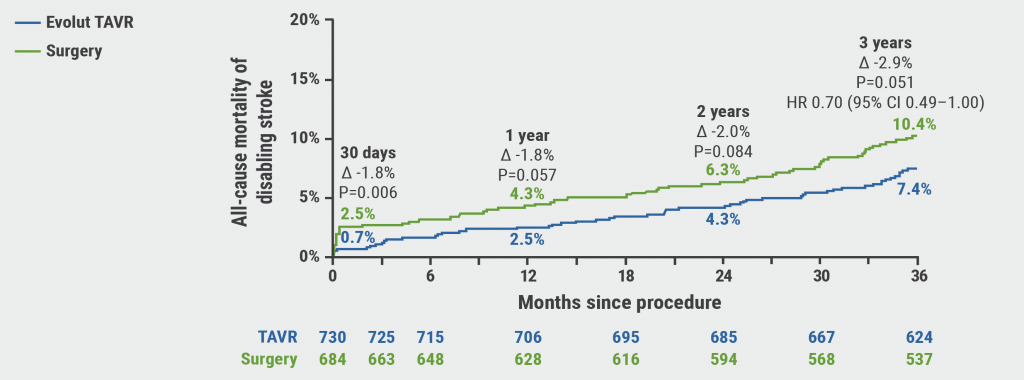
At 3 years, the primary endpoint of all-cause mortality or disabling stroke had occurred in 7.4% of the TAVR group and 10.4% of the surgery group. At 30 days, the difference between treatment arms was already -1.8%, and this remained broadly consistent over time (see Figure). All-cause mortality was 6.3% for TAVR and 8.3% for surgery (Plog-rank=0.16). The respective percentages for disabling stroke were 2.3 and 3.4 (Plog-rank=0.19).
Figure: Primary endpoint of all-cause mortality or disabling stroke [1]
Mild paravalvular regurgitation (20.3% TAVR vs 2.5% surgery) and pacemaker placement (23.2% TAVR vs 9.1% surgery; P<0.001) were less frequent in the surgery group compared with TAVR. Rates of moderate or greater paravalvular regurgitation for both groups were <1%. The TAVR group showed significantly improved valve haemodynamics, with a mean gradient of 9.1 mmHg compared with 12.1 mmHg in the surgery group (P<0.001).
Prof. Forrest concluded that “the excellent valve performance and durable outcomes up to 3 years affirm the role of TAVR with the Evolut valve in this low-risk population.”
- Forrest J, et al. Transcatheter versus surgical aortic valve replacement in aortic stenosis patients at low surgical risk: 3-year outcomes from the Evolut Low Risk trial. Session 405-14, ACC Scientific Session 2023, 4–6 March, New Orleans, USA.
- Forrest JK, et al. J Am Coll Cardiol. 2022;79(9):882–896.
Copyright ©2023 Medicom Medical Publishers
Posted on
Table of Contents: ACC 2023
Featured articles
Pulmonary Arterial Hypertension
Sotatercept improves exercise capacity in patients with PAH
Fixed-dose macitentan plus tadalafil superior to either agent alone in PAH
Coronary Revascularisation
Immediate complete revascularisation non-inferior to staged complete revascularisation
RENOVATE-COMPLEX-PCI results support intravascular-guided PCI for complex lesions
Heart Failure and Cardiomyopathy
No need to restrict vigorous exercise in selected HCM patients?
No difference in CV outcomes between PET or CMR and SPECT
Interventional and Structural Cardiology
Benefits of MitraClip sustained to 5 years in COAPT trial
Transcatheter repair for patients with tricuspid regurgitation
Minimally invasive versus conventional sternotomy for mitral valve repair
Durable benefits of TAVR versus surgical aortic valve replacement in aortic stenosis patients
PCI not better than GDMT in severe ischaemic cardiomyopathy
Prevention
Anticoagulation in non-critically ill hospitalised COVID patients
Statins associated with reduced heart dysfunction from anthracyclines
Multifaceted strategy improves prescription of therapies for diabetes and ASCVD
Dyslipidaemia
Bempedoic acid benefits statin-intolerant patients at high cardiovascular risk
Evolocumab improves coronary plaque morphology in stable CAD
Inflammation stronger predictor of MACE than cholesterol levels
Oral PCSK9 inhibitor significantly lowers LDL-C
Miscellaneous
Baxdrostat in patients with uncontrolled hypertension
Hormone therapy for gender dysphoria associated with increased CV risk
Pulsed-field ablation appears safe and effective for atrial fibrillation
Key correlates of incident dementia identified in the MESA study
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy