
https://doi.org/10.55788/f4a89ca9
Factor XI inhibition is hypothesised to reduce the risk of the development of pathological thrombi. In addition, since thrombin can still be formed with factor XI inhibition, it is expected that beneficial blood clots can be formed to prevent bleeding. In contrast, factor Xa inhibitors reduce the risk for pathological thrombi but also hamper thrombin production. The phase 2 PACIFIC-AF trial (NCT04218266) is part of the larger phase 2 PACIFIC programme, which aims to assess asundexian, a small, orally administered factor XI inhibitor [1]. The safety results were published a few days after the presentation in the Lancet [2].
In the PACIFIC-AF trial, 755 patients with AF were randomised 1:1:1 to 50 mg asundexian, 20 mg asundexian, or the factor Xa inhibitor apixaban. The primary safety endpoint was ISTH major and clinically relevant non-major (CRNM) bleeding after 12 weeks. Prof. Manesh Patel (Duke University School of Medicine, NC, USA) presented the results.
After 12 weeks, the risk of ISTH major bleeding or CRNM bleeding was lower in the pooled asundexian arms than in the apixaban arm (ratio of incidence proportion 0.33; 90% CI 0.09–0.97). The corresponding ratios of incidence proportion in the 20 mg arm and 50 mg arm were 0.50 (90% CI 0.14–1.68) and 0.16 (90% CI 0.01–0.99), respectively. Notably, no major bleedings had occurred in any treatment arm, meaning that the incidence of CRNM bleedings drove the primary safety outcome of this study. Furthermore, ISTH minor bleedings occurred more frequently in patients on apixaban than in patients on asundexian (0.42; 90% CI 0.26–0.67).
Asundexian was well tolerated in this population and no notable safety differences were reported between the 2 asundexian arms (see Figure). The rate of any adverse events (AEs) was similar for patients on asundexian (47.3%) and apixaban (48.8%) and the rates of AEs leading to discontinuation were 6.2% and 5.2% for patients receiving asundexian and apixaban, respectively. In an exploratory efficacy analysis, 0 patients in any group experienced systemic embolism. Ischaemic strokes were observed in 2 patients (0.8%) and 1 patient (0.39%) in the asundexian 20 mg and 50 mg groups, respectively, versus 0 in the apixaban arm. No conclusion can be drawn from these data at this time.
Figure: Primary safety outcome for PACIFIC-AF suggested that there was less bleeding in the arms treated with asundexian versus apixaban [1]
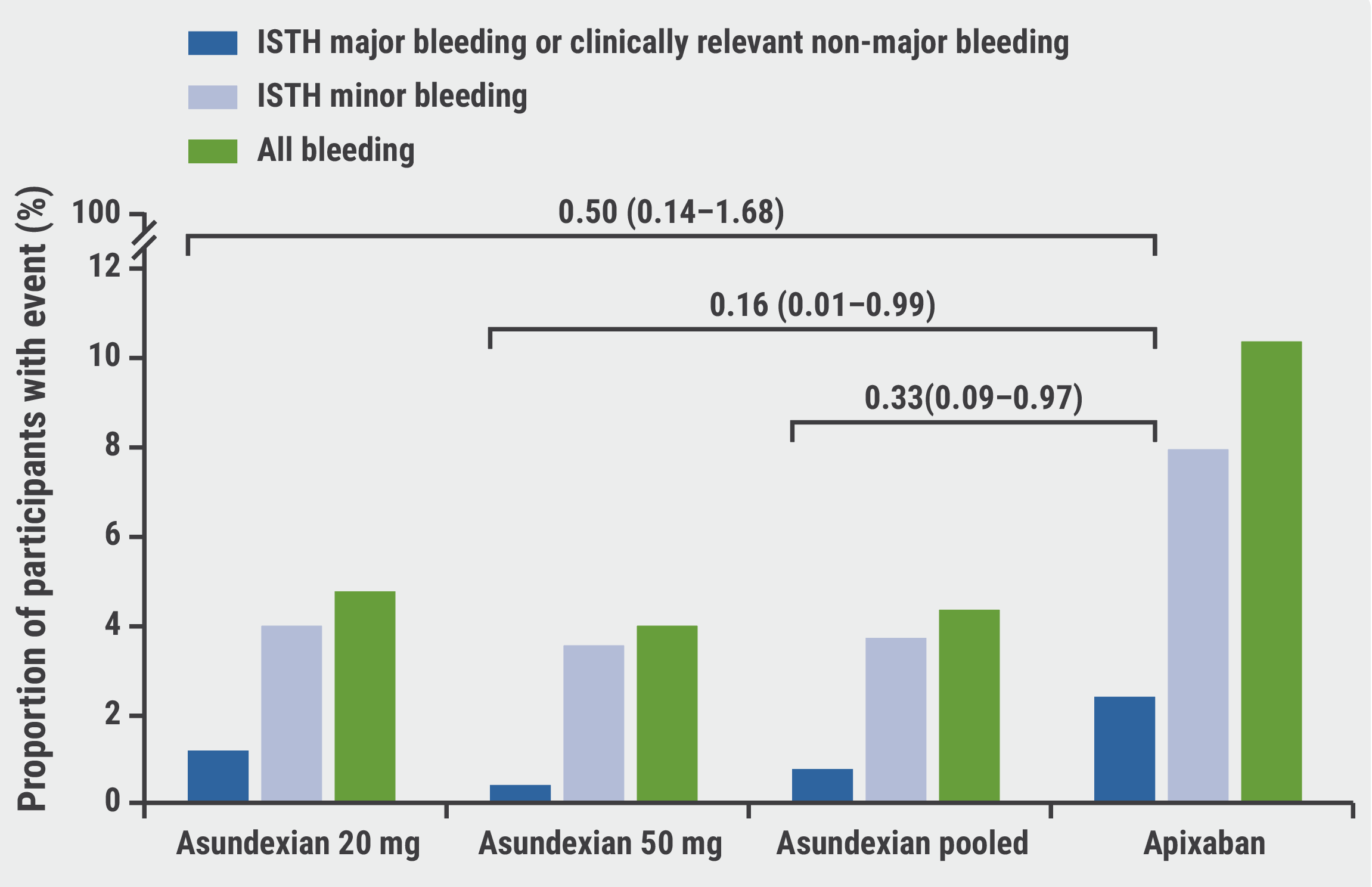
ISTH, International Society on Thrombosis and Haemostasis.
Asundexian is a promising agent that may provide thromboembolic protection with a more favourable safety profile relative to existing anticoagulants; however, phase 3 trials are needed to validate the findings of this study and provide data on the efficacy of asundexian.
- Patel MR, et al. Multicenter, Randomized, Active Comparator-Controlled, Double-Blind, Double-Dummy, Parallel Group, Dose-Finding Phase 2 Study Comparing the Safety of the Oral FXI1 Inhibitor Asundexian with Apixaban in Patients with Atrial Fibrillation: PACIFIC-AF. Abstract 407–08, ACC 2022, 2–4 April, Washington DC, USA.
- Piccini JP, et al. Lancet. 2022;399(10333):1383–1390.
Copyright ©2022 Medicom Medical Publishers
Posted on
Table of Contents: ACC 2022
Featured articles
Alirocumab significantly reduces high-risk coronary plaques
Highlighted Original Research
POISE-3: Tranexamic acid for non-cardiac surgery
Treating chronic mild hypertension during pregnancy leads to better outcomes
New VOYAGER PAD data: Should patients with both PAD and CKD get rivaroxaban?
Alirocumab significantly reduces high-risk coronary plaques
Aggressive warming during non-cardiac surgery does not improve outcomes
Heart Failure and Cardiomyopathy
DIAMOND trial: Patiromer lowers risk of severe hyperkalaemia
Replacing septal reduction therapy with mavacamten for HCM
Omecamtiv mecarbil does not impact exercise capacity of patients with HFrEF
Symptomatic obstructive hypertrophic cardiomyopathy: long-term mavacamten control
Interventional and Structural Cardiology
COMPLETE revascularisation improves angina-related QoL
Plot twist for negative FAME 3 results: early QoL benefits of PCI
1-year CLASP TR results support tricuspid regurgitation repair
Head-to-head: post-TAVR edoxaban not better than DAPT
Chocolate Touch vs Lutonix catheters
No FLAVOUR difference between FFR and IVUS for PCI guidance
Myocardial Infarction
Low-resource countries benefit from global STEMI initiative
Sodium thiosulfate ineffective at cardiac protection
ICM-guided management did not improve MACE after MI
Prevention
PACIFIC-AF: Low bleeding rates for asundexian in atrial fibrillation
RCT-IVVE trial: Do HF patients benefit from annual flu shots?
TRANSLATE-TIMI 70: Primary endpoint met but safety concerns for vupanorsen
Lipoprotein(a) slashed by 98% in APOLLO trial
Dietary intervention from your supermarket

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com