
It is widely known that osteoporosis and vertebral fractures are common comorbidities of axSpA, as well as the fact that they have deleterious effects on patients’ physical function. It was recently shown by Romera-Lopez et al. that in those patients, low femoral neck bone mineral density (BMD) is associated with disease activity and vitamin D insufficiency and vertebral fractures are associated with CRP and low hip bone mass density.
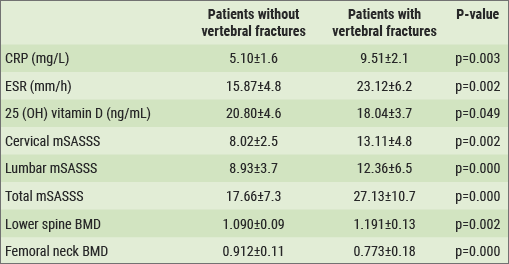
This relationship between disease activity and radiographic damage and BMD, 25 (OH) vitamin D levels and vertebral fractures in patients with axSpA was evaluated in a cross-sectional study, involving 206 patients. The majority was male (144 men/62 women), and 86% had AS, 14% nr-axSpA, and associated peripheral involvement was seen in 42%. Mean age was 52 years and mean BASDAI was 3.6, mean ASDAS-CRP 2.2, mean ASDAS-ESR 2.5, mean CRP 4.97 mg/L, mean ESR 18 mm. With regard to physical function, mean BASFI was 3.3; radiographic progression: mean mSASSS total was 20.46, lumbar 10.41, and cervical 10.05. It emerged that 85.7% of patients had insufficient levels of 25 (OH) vitamin D (mean 19.83 ng/mL). Low lumbar spine BMD was seen in 25.7% (z-score) and 28.9% (t-score), and low femoral neck BMD occurred in 45.2% (z) and 28.9% (t) of the patients. The prevalence of osteoporosis in lumbar spine was 3.2% (z)/6.9% (t) and in femoral neck 9.1% (z)/13.4% (t). Morphometric vertebral fractures were identified in 34% of the patients. Bivariate analysis demonstrated that ESR, ASDAS-ESR, age, male sex, low 25 (OH) vitamin D levels, and the mSASSS were associated with low femoral neck BMD. Multivariate models confirmed the association between disease activity (assessed by ASDAS-ESR OR 3.32; 95% CI 2.35-4.55; p=0.016), 25(OH) vitamin D (OR 0.95; 95% CI 0.86-0.98; p=0.029) and low femoral neck BMD (z-score). An association was confirmed between CRP (OR 2.34; 95% CI 1.10-4.98; p=0.027), radiographic damage (lumbar mSASSS OR 1.06; 95% CI 1.03-1.10; p=0.001), high lumbar spine BMD (OR 296; 95% CI 5.07-12258; p=0.006), and low femoral neck BMD (OR 0.11; 95% CI 0.03-0.12; p=0.000) and the presence of vertebral fractures (see Table).[1] It should be noted that the association with high lumbar spine BMD might be related to the presence of radiographic damage, or to effects of new bone formation in the lumbar spine.
Table: Differences in parameters in axSpA patients with/without vertebral fractures[1]
- Romera-Lopez C, et al. Abstract OP0065. EULAR 2018.
Posted on
Table of Contents: EULAR 2018
Featured articles
Rheumatoid Arthritis
Switching to biosimilar bDMARDs is safe and efficacious
No significant differences when tapering TNF blockers versus csDMARDs
Confirmation of long-term safety profile adalimumab across indications
Ankylosing Spondylitis
Clinical effect of vedolizumab on articular manifestations spondyloarthritis associated with IBD
Synergistic effect NSAIDs plus TNFi in slowing radiographic progression in ankylosing spondylitis patients
Osteoporosis and Osteoarthritis
Systemic Sclerosis and Systemic Lupus Erythematosus
Promising results rituximab in systemic sclerosis, and systemic lupus erythematosus classification criteria
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com