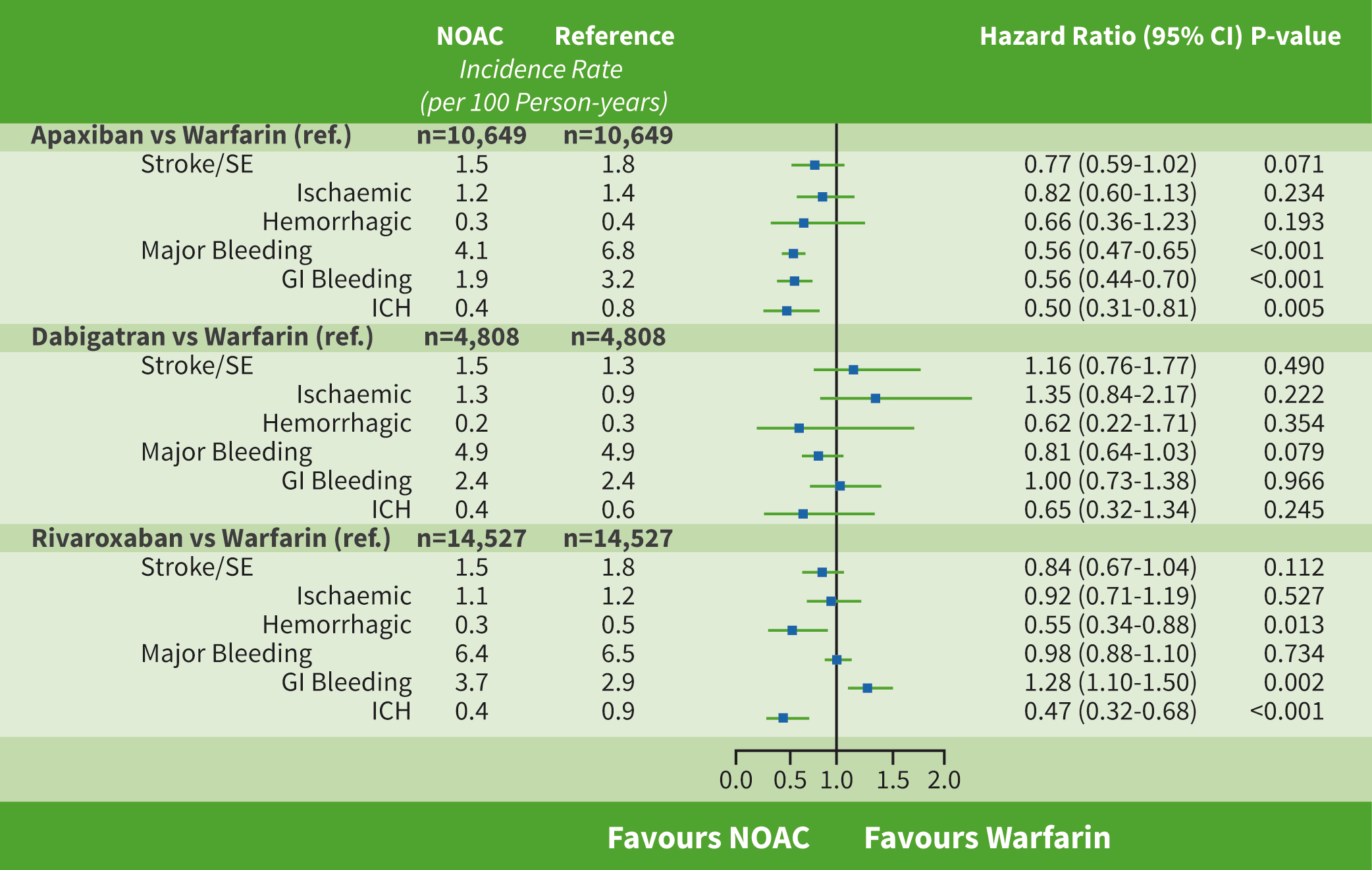
These results, presented by Dr Steven Deitelzweig (Ochsner Health System, USA), were derived from the ARISTOPHANES population and pooled CMS Medicare data with 4 US commercial claims databases. This covers >180 million beneficiaries annually (approximately 56% of the US population). A total of 62,143 obese patients (19.3 %) with non-valvular AF were included: 13,130 (21.1%) on apixaban, 5,349 (8.6%) on dabigatran, 20,278 (32.6%) on rivaroxaban, and 23,386 (37.6%) on warfarin. Propensity score matching was used to balance baseline characteristics between patients prescribed each DOAC and warfarin: apixaban (n=10,649)-warfarin (n=10,649), dabigatran (n=4,808)-warfarin (n=4,808), and rivaroxaban (n=14,527)-warfarin (14,527). Before propensity score matching, warfarin patients were the oldest and had the highest CCI, CHA2DS2-VASc, and HAS-BLED scores compared with DOAC patients. The mean follow-up time ranged between 6 and 8 months. Mean ages were 71, 69, and 71 years for the apixaban-warfarin, dabigatran-warfarin, and rivaroxaban-warfarin cohort pairs, respectively. The mean CHA2DS2-VASc scores were 3.9, 3.7, and 3.9 for the apixaban-warfarin, dabigatran-warfarin, and rivaroxaban-warfarin cohort pairs, respectively. The results are outlined in the Table below.
Figure: Comparison of stroke/SE and major bleeding rate [1]
Limitations of the study include propensity score matching being conducted between each cohort pair, which means the results are not comparable across all matched populations. Also, only associations could be concluded from this study as there are potential residual confounders such as over-the-counter use of aspirin or warfarin treatment dose change.
1. Deitelzweig S, et al. J Am Coll Cardiol. 2019;73(9):435. DOI: 10.1016/S0735-1097(19)31043-5.
Posted on
Table of Contents: ACC 2019
Featured articles
Acute and Stable Ischaemic Heart Disease
Arrhythmias and Clinical Electrophysiology
Substantial impact of temporary interruptions of warfarin versus DOAC
Smartwatch can detect atrial fibrillation with high degree of accuracy
Congenital Heart Disease
Heart Failure and Cardiomyopathies
Frequent use of beta-blocker after HFpEF hospitalisations in elderly patients without compelling indications
High 5-year survival rates for older HF patients without initial severe comorbidity
Pulmonary Arterial Hypertension and Venous Thromboembolism
Interventional Cardiology
Vascular Medicine
Lower rates stroke/SE with DOACs in frail non-valvular AF patients
Similar rates of stroke/SE associated with DOAC vs warfarin use in obese non-valvular AF patients: Results from an observational registry
Convincing evidence of the role of icosapent in reducing subsequent CV events
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy