
Ponesimod is an orally active, selective S1P1-receptor modulator that induces rapid, dose-dependent, and reversible reductions in peripheral blood lymphocyte count. In the phase 3 OPTIMUM study (NCT02425644), ponesimod 20 mg demonstrated superior efficacy versus teriflunomide 14 mg in reducing annualised relapse rate (ARR) in patients with relapsing MS [1]. Cases of exacerbation of MS activity have been reported after discontinuation of S1P1-receptor modulators.
Prof. Ludwig Kappos (University of Basel, Switzerland) reported on the post-treatment relapse activity in the OPTIMUM study [2]. He explained that all patients who completed treatment in the OPTIMUM study after 108 weeks, regardless of treatment group, interrupted treatment for at least 2 weeks and, for teriflunomide, underwent an accelerated elimination procedure. All patients who stopped treatment, either prematurely or not, entered safety follow-up (at least 30 days after the last dose), and a post-treatment observation period (from the last dose up to 108 weeks after randomisation).
Of 1,133 randomised patients, 1,124 had post-treatment observation. In the ponesimod and teriflunomide group, 88 and 92 patients stopped treatment prematurely, respectively. Eight patients in the ponesimod group and 14 in the teriflunomide group experienced a total of 23 post-treatment relapses within 182 days of the last received dose of either study drug. Post-treatment ARR did not exceed on-treatment ARR for both drugs. Including non-confirmed relapses, ARR in the ponesimod group was 0.246 on-treatment, and 0.186 off-treatment; ARR in the teriflunomide group was 0.348 and 0.294, respectively. These findings are consistent with the main OPTIMUM results up to the end of the study. There were 8 confirmed on-treatment relapses in 5 ponesimod-treated patients, and 9 relapses (3 confirmed) in 8 patients between 6 and 168 days post-treatment, without any pattern of latency or severity.
- Kappos L, et al. JAMA Neurol. 2021 May 1;78(5):558-67.
- Kappos L, et al. Analysis of post-treatment relapse activity in the phase 3 OPTIMUM study of ponesimod compared with teriflunomide. OPR-208, EAN 2021 Virtual Congress, 19–22 June.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: EAN 2021
Featured articles
Letter from the Editor
COVID-19
First evidence of brainstem involvement in COVID-19
Cognitive/behavioural alterations persistent after COVID-19
Neural base of persistent hyposmia after COVID-19
Neurological symptoms and complications of COVID-19 affect outcomes
Cerebrovascular Disease
Intracerebral haemorrhage only slightly increases mortality in COVID-19 patients
Stroke with covert brain infarction indicates high vascular risk
Expanding precision medicine to stroke care
Dexamethasone not indicated for chronic subdural haematoma
Cognitive Impairment and Dementia
Severe outcomes of COVID-19 in patients with dementia
Promising diagnostic accuracy of plasma GFAP
Sex modulates effect of cognitive reserve on subjective cognitive decline
Hypersensitivity to uncertainty in subjective cognitive decline
Epilepsy
Minimally invasive device to detect focal seizure activity
‘Mozart effect’ in epilepsy: why Mozart tops Haydn
Migraine and Headache
Factors associated with decreased migraine attack risk
Pregnant migraine patients at higher risk of complications
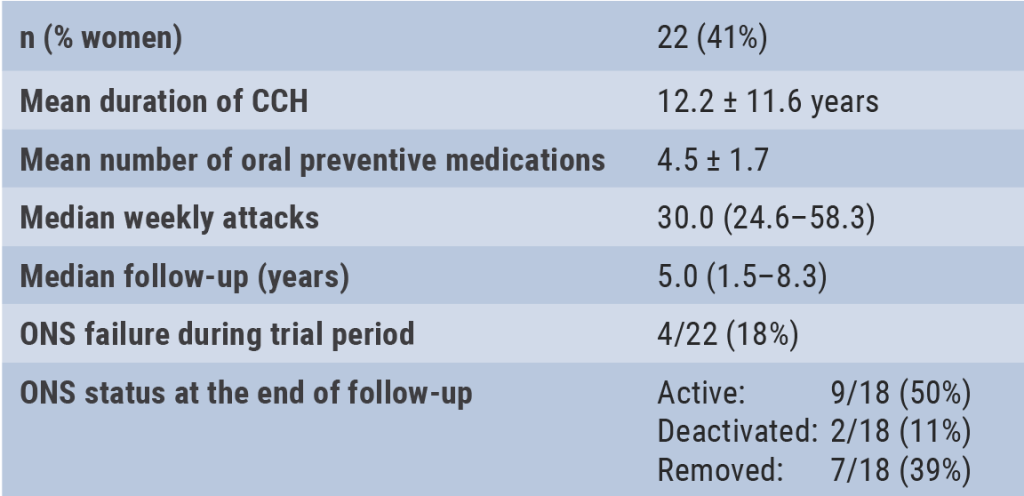
Occipital nerve stimulation in drug-resistant cluster headache
Rhythmicity in primary headache disorders
Multiple Sclerosis and NMOSD
Typing behaviour to remotely monitor clinical MS status
Alemtuzumab in treatment-naïve patients with aggressive MS
No higher early MS relapse frequency after stopping ponesimod
Good long-term safety and efficacy of inebilizumab in NMOSD
Neuromuscular Disorders
Inability to recognise disgust as first cognitive symptom of ALS
Pathogenic T-cell signature identified in myasthenia gravis
Parkinson’s Disease
Levodopa-carbidopa intestinal gel in patients with advanced PD
New Frontier – Navigated Transcranial Ultrasound
Exploring the possibilities
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com