
https://doi.org/10.55788/b6a51cc5
“In Crohn’s disease, there is a decline in resection rates but not in re-resection rates,” expressed Dr Anja Poulsen (Copenhagen University, Denmark) [1]. The current population-based study aimed to describe the re-resection rates for patients with CD and to identify disease-modifying factors and risk factors associated with disease recurrence and re-resection. The authors identified 631 Danish patients who had undergone primary resection for CD [2].
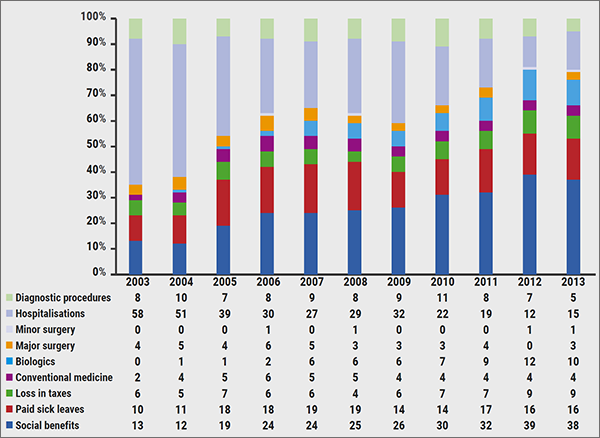
“The cumulative risk of re-resection due to disease activity was 3.6% at 1 year, 10.1% at 5 years, and 14.1% at 10 years,” stated Dr Poulsen. Also, the median time from primary resection to disease recurrence was 11.0 months, with corresponding disease recurrence rates of 36.9% at 1 year, 66.1% at 5 years, and 73.6% at 10 years (see Figure). Next, Dr Poulsen mentioned that the most commonly performed resections were a ‘simple ileocecal resection’ (60.0%), an ‘ileocecal resection with colon ascendens included’ (10.0%), and a ‘more extensive ileocecal resection’ (7.8%). “Importantly, patients undergoing a simple ileocecal resection as primary surgery had a re-resection risk of 6.3%, whereas those who underwent a small bowel resection or had a part of the colon included in the primary resection had re-resection risks of 14.3% and 19.0%, respectively. Furthermore, there was a reduced risk of re-resection in patients with B2 or B3 disease types who received biological therapy within the first year after primary resection (B2: HR 0.56; 95% CI 0.34–0.93; P=0.026; B3: HR 0.31; 95% CI 0.15–0.64; P=0.002). Finally, prophylactic biological therapy after a primary ileocecal resection appeared to reduce the risk of post-operative disease recurrence and re-resection (HR 0.58; 95% CI 0.34–0.99; P=0.047).
Figure: Time from primary resection to disease recurrence [2]

CTA, computed tomography angiography; IUS, intestinal ultrasonography; MRI, magnetic resonance imaging; SES-CD, simple endoscopic score for Crohn’s disease.
The current study provided insights into re-resection rates and associated risk factors in patients with CD. Disease phenotype, involved segments in the primary resection procedure, and biological therapies appear to influence the risk of disease recurrence and re-resection in these patients.
- Tsai L, et al. Clin Gastroenterol Hepatol. 2021;19(10):2031-2045.e11.
- Poulsen A, et al. Risk of disease recurrence and re-resections in Crohn’s disease patients undergoing primary bowel resection: a population-based study. OP34, 19th Congress of ECCO, 21–24 February 2024, Stockholm, Sweden.
Copyright ©2024 Medicom Medical Publishers
Posted on
Table of Contents: ECCO 2024
Featured articles
Meet the Trialist: Dr Yasuharu Maeda on AI-assisted endoscopy
IL-23 Inhibitors on the Rise
VIVID-1: Mirikizumab meets expectations in Crohn’s disease
COMMAND: Long-term efficacy benefits of risankizumab in ulcerative colitis
SEQUENCE: Risankizumab versus ustekinumab across endpoints
QUASAR: Guselkumab improves QoL for patients with ulcerative colitis
Fatigue, urgency, and QoL improvements on mirikizumab in Crohn’s disease
Inspiring Drug Trials and Treatment Strategies
Novel agent VTX002 holds promise in ulcerative colitis
PROFILE: Top-down treatment strategy benefits patients with early Crohn’s disease
Biologicals and JAK inhibitors hold promise in microscopic colitis
Ustekinumab as alternative for anti-TNFs in HLA-DQA1*05-positive Crohn’s disease
How effective is dose escalation of biologicals in IBD?
Make Way for JAK Inhibitors
Promising data for JAK inhibitors in Crohn’s disease from phase 2 trial
U-ENDURE long-term extension: sustained efficacy of upadacitinib in Crohn’s disease
TRIUMPH: Tofacitinib as rescue option for acute severe ulcerative colitis
Focus on Endoscopy, Screening, and Risk Factors
Should we screen for metabolic bone disease at IBD diagnosis?
Predicting relapse in ulcerative colitis with AI-assisted endoscopy
Clear case for NUDT15 genetic testing in Asian patients with IBD
HELIOS: HD-WLE can yield similar neoplasia detection rates as HD-CE
CURE-CD: Capsule endoscopy-guided proactive treatment leads to fewer relapses in Crohn’s disease
Sharp Surgical Solutions
Extended mesenterectomy or mesenteric-sparing surgery in Crohn’s disease?
Similar outcomes for Kono-S and side-to-side anastomosis in Crohn’s terminal ileitis
Risk factors for re-resection in Crohn’s disease revealed
ADMIRE-CD-II: Darvadstrocel does not meet primary endpoint in complex peri-anal fistula

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com