
https://doi.org/10.55788/c9ec2496
Adjuvant therapy with the CDK4/6 inhibitor abemaciclib combined with endocrine therapy demonstrated significant improvement in invasive disease-free survival (IDFS) and distant recurrence-free survival (DRFS) in high-risk, HR-positive/HER2-negative, node-positive early breast cancer after 2 years of follow-up [1,2]. To evaluate the efficacy of abemaciclib after completion of the therapy, an analysis was completed 2 years after the primary outcome analysis. Prof. Stephen Johnston (The Royal Marsden NHS Foundation Trust, UK) presented the results of this analysis [3,4].
The phase 3 monarchE trial (NCT03155997) enrolled 5,637 patients who were 1:1 randomised to receive abemaciclib for 2 years plus endocrine therapy (≥5 years) or endocrine therapy alone. All patients were high-risk based on either clinical pathological features (Cohort 1, n=5120) or on the Ki-67 test (Cohort 2, n=517). After a median follow-up of 42 months, IDFS curves between the 2 treatment arms continued to widen in favour of abemaciclib. The absolute benefit of abemaciclib in IDFS 4-year rate was 6.4% compared with 2.8% after 2 years and 4.8% after 3 years of follow-up. HR for IDFS improved from 0.782 in the first year of follow-up to 0.602 after 4 years of follow-up.
Likewise, DRFS benefit of abemaciclib persisted beyond completion of abemaciclib: The absolute benefit of abemaciclib in DRFS 4-year rate was 5.9% compared with 2.5% after 2 years and 4.1% after 3 years of follow-up. HR for DRFS improved from 0.725 in the first year of follow-up to 0.581 after 4 years of follow-up. Addition of abemaciclib to endocrine therapy did improve IDFS and DFRS both in Cohort 1 and Cohort 2. Ki-67 score showed to be prognostic for a poor outcome, but not predictive of abemaciclib efficacy. Although the overall survival data are not yet mature, there was a numerical difference in deaths (157 vs 173) and number of patients with metastatic disease (125 vs 249) in favour of the abemaciclib arm.
“These data further support the addition of adjuvant abemaciclib to endocrine therapy for patients with HR-positive/HER2-negative, node-positive, high-risk early breast cancer,” concluded Prof. Johnston.
- Johnston SRD, et al. J Clin Oncol. 2020;38:3987–3998.
- Harbeck N, et al. Ann Oncol. 2021;32:1571–1581.
- Johnston SRD, et al. Abemaciclib plus endocrine therapy for HR+, HER2-, node-positive, high-risk early breast cancer: results from a pre-planned monarchE overall survival interim analysis, including 4-year efficacy outcomes. Abstract GS1-09, SABCS 2022, 6–10 December, San Antonio, TX, USA.
- Johnston SRD, et al. Lancet Oncol. 2023;24(1):77–90.
Copyright ©2023 Medicom Medical Publishers
Posted on
Table of Contents: SABCS 2022
Featured articles
Miscellaneous
Racial disparity in the tumour microenvironment
Chemo-endocrine therapy worse for cognition than endocrine therapy alone
Early-Stage Breast Cancer
Anti-PD-1/anti-LAG-3 combination highly effective in HER2-negative breast cancer
MammaPrint test predictive for benefit of extended endocrine therapy
HR-positive/HER2-positive Breast Cancer: Trastuzumab-Deruxtecan
Trastuzumab deruxtecan effective in both second-line and neoadjuvant setting
HR-positive/HER2-negative Advanced Metastatic Breast Cancer
Benefit of adjuvant abemaciclib continues to deepen at longer follow-up
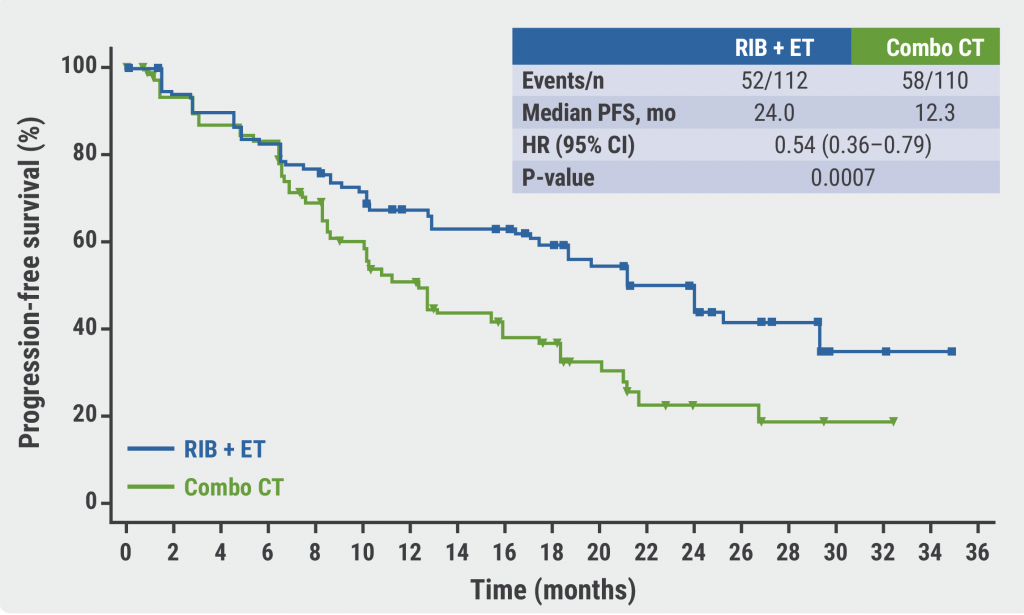
First-line ribociclib plus endocrine therapy outperforms combination chemotherapy
Treatment options beyond CDK4/6 inhibition
Triple-Negative Breast Cancer
Baseline CTC count can guide first-line treatment in HR-positive/HER-negative metastatic breast cancer
ZNF689 deficiency promotes intratumour heterogeneity and resistance to immune checkpoint blockade in TNBC
Oestradiol represses anti-tumoural immune response to promote progression of brain metastases
Basic and Translational Research
Resistance to CDK4/6 inhibitors is likely due to expansion of pre-existing resistant clones
Germline pathogenic variants for breast cancer also increase contralateral breast cancer risk
Low-dose tamoxifen still prevents recurrence from non-invasive breast cancer
Endocrine interruption to pursue pregnancy does not impact short-term disease in breast cancer
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com