
Neuroblastoma is the most common extracranial solid tumour in paediatrics. High-risk disease comprises about half of all diagnoses and long-term survival is poor. Plasma ctDNA has been demonstrated to be present at high levels in neuroblastoma and provides an important tool and surrogate for tumour molecular analyses [1].
The multicentre, open-label, randomised, phase 2 NANT2011-01 trial (NCT02035137) evaluated the diagnostic and therapeutic agent metaiodobenzylguanidine (MIBG) with or without radiation sensitisers for patients with relapsed or refractory neuroblastoma. In a pre-planned exploratory analysis, presented by Dr Kevin Campbell (Dana-Farber Cancer Institute, MA, USA), plasma samples from the NANT2011-01 trial, were used to evaluate the potential use of ctDNA as a biomarker to evaluate response to MIBG [2]. Plasma was collected at baseline prior to MIBG and at 4, 5, 15, and 50 days after MIBG. Samples were analysed for percentage ctDNA levels using ultra-low passage whole-genome sequencing.
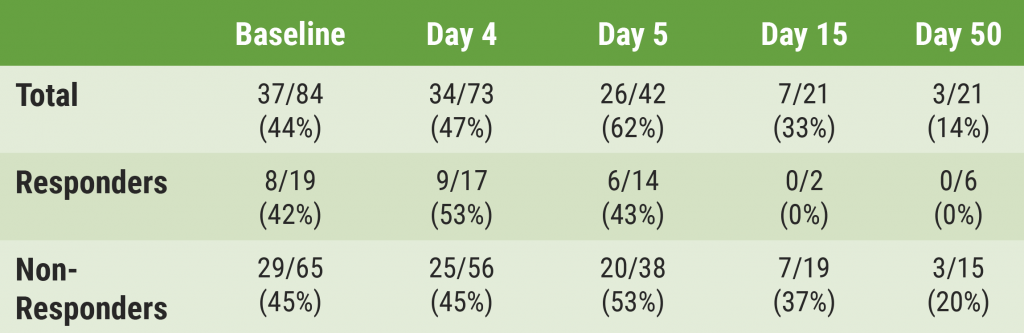
This analysis included 84 patients with a median age of 6.25 years. Of the 37 patients (44%) with detectable ctDNA at baseline, the median ctDNA level was 32%. Baseline ctDNA levels showed a significant positive correlation with percentage involvement in bone marrow and Curie score but not RECIST sum of diameters for soft tissue sites. Following therapy, the proportions of patients with detectable ctDNA were 47% at day 4, 62% at day 5, 33% at day 15, and 14% at day 50. The rate of ctDNA detection was similar between responders and non-responders at baseline, day 4, and day 5, but undetectable in responders at day 15 and day 50 versus 37% and 20% in non-responders (see Table).
Table: Proportion of patients with detectable ctDNA according to response to first course [2]
Dr Campbell concluded that these results warrant further use of ctDNA to evaluate the response to treatment in children with relapsed or refractory neuroblastoma. For example, it should be investigated how copy number alterations or segmental chromosomal aberrations detectable in ctDNA might be associated with differential response to MIBG therapy.
- Klega K, et al. JCO Presic Oncol. 2018;2:PO.17.00285.
- Campbell KM, et al. Changes in ctDNA levels after MIBG therapy in patients with relapsed or refractory neuroblastoma. Abstract 10012, ASCO 2021 Virtual Meeting, 4–8 June.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: ASCO 2021
Featured articles
Downloadable 1-Page Editor-Selected Trial PowerPoint Slides
Breast Cancer
Excellent prognosis for breast cancer patients with ultra-low-risk gene signature
Olaparib benefits early breast cancer patients with BRCA1/2 germline mutation
Platinum-based adjuvant chemotherapy in TNBC is not superior or non-inferior to capecitabine
Dalpiciclib benefits patients with HR-positive, HER2-negative advanced breast cancer
Trastuzumab-deruxtecan showed clinical activity in patients with brain metastases
Lung Cancer
Neoadjuvant nivolumab plus chemotherapy improves surgical outcomes in NSCLC
Immune-related adverse events are associated with efficacy of atezolizumab in patients with advanced NSCLC
Sustained efficacy of nivolumab/ipilimumab plus 2 cycles of chemotherapy in NSCLC
Patritumab deruxtecan (HER3-DXd) in EGFR TKI-resistant NSCLC
Melanoma
Long-term results from ground-breaking melanoma trials
Novel dual checkpoint blockade improves progression-free survival in melanoma
Neoadjuvant therapy with nivolumab plus relatlimab is safe and effective in patients with stage III melanoma
Genitourinary Cancers
VISION trial shows improved survival with 177Lu-PSMA-617 in mCRPC
Abiraterone added to ADT + docetaxel nearly doubles survival in de novo mCSPC
Post-nephrectomy pembrolizumab improves disease-free survival
Glutaminase inhibitor telaglenastat does not improve survival mRCC
Promising efficacy and safety of feladilimab in recurrent/metastatic urothelial carcinoma
Gastrointestinal Cancers
Pembrolizumab benefits survival in MSI-H/dMMR metastastic colorectal cancer
Panitumumab added to 5-FU/LV effective as maintenance therapy in patients with mCRC
Trastuzumab-deruxtecan showed promising activity in patients with HER2-expressing mCRC
Benefit of both I-O/chemo combo and I-O/I-O combo over chemotherapy alone in oesophageal squamous cell cancer
Benefit of I-O/chemo combo over chemotherapy alone in advanced GC/GEJC/EAC
Perioperative chemotherapy and neoadjuvant multimodality therapy appear equally effective
Haematological Cancers
Olutasidenib demonstrates efficacy in patients with relapsed/refractory IDH1 mutant AML
Acalabrutinib as effective but better tolerated than ibrutinib in CLL
Gynaecological Cancers
Adjuvant chemotherapy does not improve outcome in patients with locally advanced cervical cancer
Novel drug combination for recurrent ovarian cancer
Dual HER2-blockade shows anti-tumour activity in patients with uterine cancer
Paediatric Cancer
Molecular tumour profiling impacts the diagnosis and treatment of solid tumours
Circulating tumour DNA to evaluate response in children with neuroblastoma
Basic Science
PARP7 inhibitor shows promising results in first-in-human trial
IACS-6274 is well tolerated and biologically active in selected advanced tumours
CYT-0851 shows promising anti-tumour activity across different tumour types
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com