
Bruton tyrosine kinase (BTK) is critical for CLL tumour cell proliferation and survival [1]. Ibrutinib, the first BTK inhibitor approved for adults with CLL, is associated with adverse events, particularly cardiovascular toxicities, that can lead to treatment discontinuation [2].
The randomised, non-inferiority, phase 3 ELEVATE-RR trial (NCT02477696) compared ibrutinib and acalabrutinib, a second-generation BTK inhibitor, in previously treated patients with CLL requiring therapy. The study randomised 533 patients 1:1 to receive acalabrutinib (100 mg twice daily) or ibrutinib (420 mg once daily) until progression or unacceptable toxicity. The primary endpoint was progression-free survival; secondary endpoints were incidence of all-grade atrial fibrillation, grade ≥3 infection, Richter transformation, and overall survival. Prof. John Byrd (Ohio State University Comprehensive Cancer Center, OH, USA) presented the first results of this head-to-head trial [3].
At a median follow-up of 40.9 months, progression-free survival was 38.4 months in both arms (HR 1.00; 95% CI 0.79-1.27), so the primary endpoint of non-inferiority was met. Acalabrutinib was statistically superior to ibrutinib in all-grade atrium fibrillation incidence (9.4% vs 16.0%; P=0.023). Among the other secondary endpoints, incidences of grade ≥3 infection and Richter transformation were comparable between arms. Median overall survival was not reached in either arm (HR 0.82; 95% CI 0.59–1.15), with 63 (23.5%) deaths in the acalabrutinib arm and 73 (27.5%) in the ibrutinib arm.
Acalabrutinib was associated with a lower incidence of hypertension (8.6% vs 22.8%), arthralgia (15.8% vs 22.8%), and diarrhoea (34.6% vs 46.0%), but a higher incidence of headache (34.6% vs 20.2%) and cough (28.9% vs 21.3%). Adverse events led to treatment discontinuation in 14.7% of acalabrutinib-treated patients versus 21.3% of ibrutinib-treated patients. Among any-grade events, both cardiac and bleeding events were less frequent with acalabrutinib (24.1% vs 30.0% and 38.0% vs 51.3%, respectively; see Table).
Table: Events of clinical interest [2]

- Vitale C, Burger JA. Expert Opin Pharmacother. 2016;17:1077-1189.
- Dickerson T, et al. Blood 2019;134:1919-1928.
- Byrd, JC, et al. First results of a head-to-head trial of acalabrutinib versus ibrutinib in previously treated chronic lymphocytic leukemia. Abstract 7500, ASCO 2021 Virtual Meeting, 4–8 June.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: ASCO 2021
Featured articles
Downloadable 1-Page Editor-Selected Trial PowerPoint Slides
Breast Cancer
Excellent prognosis for breast cancer patients with ultra-low-risk gene signature
Olaparib benefits early breast cancer patients with BRCA1/2 germline mutation
Platinum-based adjuvant chemotherapy in TNBC is not superior or non-inferior to capecitabine
Dalpiciclib benefits patients with HR-positive, HER2-negative advanced breast cancer
Trastuzumab-deruxtecan showed clinical activity in patients with brain metastases
Lung Cancer
Neoadjuvant nivolumab plus chemotherapy improves surgical outcomes in NSCLC
Immune-related adverse events are associated with efficacy of atezolizumab in patients with advanced NSCLC
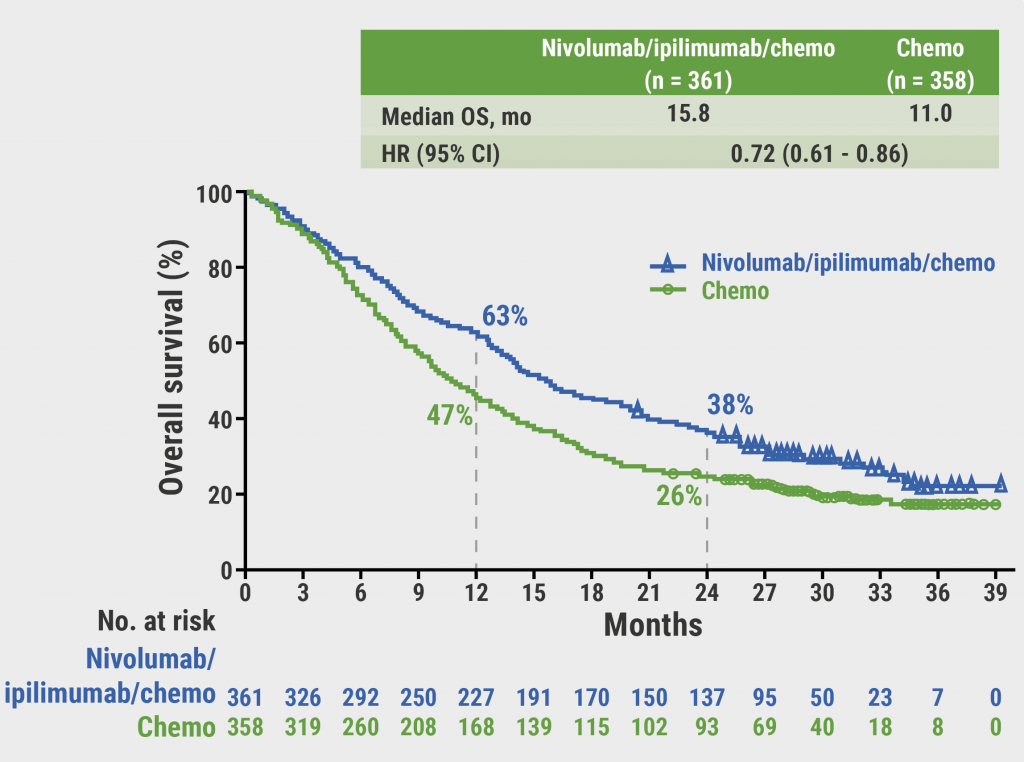
Sustained efficacy of nivolumab/ipilimumab plus 2 cycles of chemotherapy in NSCLC
Patritumab deruxtecan (HER3-DXd) in EGFR TKI-resistant NSCLC
Melanoma
Long-term results from ground-breaking melanoma trials
Novel dual checkpoint blockade improves progression-free survival in melanoma
Neoadjuvant therapy with nivolumab plus relatlimab is safe and effective in patients with stage III melanoma
Genitourinary Cancers
VISION trial shows improved survival with 177Lu-PSMA-617 in mCRPC
Abiraterone added to ADT + docetaxel nearly doubles survival in de novo mCSPC
Post-nephrectomy pembrolizumab improves disease-free survival
Glutaminase inhibitor telaglenastat does not improve survival mRCC
Promising efficacy and safety of feladilimab in recurrent/metastatic urothelial carcinoma
Gastrointestinal Cancers
Pembrolizumab benefits survival in MSI-H/dMMR metastastic colorectal cancer
Panitumumab added to 5-FU/LV effective as maintenance therapy in patients with mCRC
Trastuzumab-deruxtecan showed promising activity in patients with HER2-expressing mCRC
Benefit of both I-O/chemo combo and I-O/I-O combo over chemotherapy alone in oesophageal squamous cell cancer
Benefit of I-O/chemo combo over chemotherapy alone in advanced GC/GEJC/EAC
Perioperative chemotherapy and neoadjuvant multimodality therapy appear equally effective
Haematological Cancers
Olutasidenib demonstrates efficacy in patients with relapsed/refractory IDH1 mutant AML
Acalabrutinib as effective but better tolerated than ibrutinib in CLL
Gynaecological Cancers
Adjuvant chemotherapy does not improve outcome in patients with locally advanced cervical cancer
Novel drug combination for recurrent ovarian cancer
Dual HER2-blockade shows anti-tumour activity in patients with uterine cancer
Paediatric Cancer
Molecular tumour profiling impacts the diagnosis and treatment of solid tumours
Circulating tumour DNA to evaluate response in children with neuroblastoma
Basic Science
PARP7 inhibitor shows promising results in first-in-human trial
IACS-6274 is well tolerated and biologically active in selected advanced tumours
CYT-0851 shows promising anti-tumour activity across different tumour types
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com