
“We should not expect a ‘cure’ with single-shot treatments, and we need more academic studies to establish the role of CAR retreatment or maintenance studies,” stated Dr Mai. Furthermore, there is a need to improve bridging strategies, even in the early lines of therapy. “As a community and as physicians, we are responsible for equal access to experimental therapies post-relapse in patients treated in the standard arm of clinical trials. Authorities and physicians should thus accept that an overall survival benefit cannot be expected in multiple myeloma, but acknowledge that detrimental or inferior overall survival should not be accepted,” Dr Mai continued.
A potential dilemma is who should receive treatment with CAR T-cell therapies, considering restricted resources, including the need for a dedicated administration centre and the involved manufacturing process [3]. Should patients who derive the largest potential clinical benefit and quality-of-life be prioritised over patients with the largest medical need and who urgently need treatment? A solution to these questions could be to use the MyCARe model which predicts which patients are at the highest risk of early relapse following CAR T-cell therapies based on factors of early relapse such as presence of extramedullary disease, high-risk cytogenetics, ferritin levels, and lenalidomide refractoriness [4].
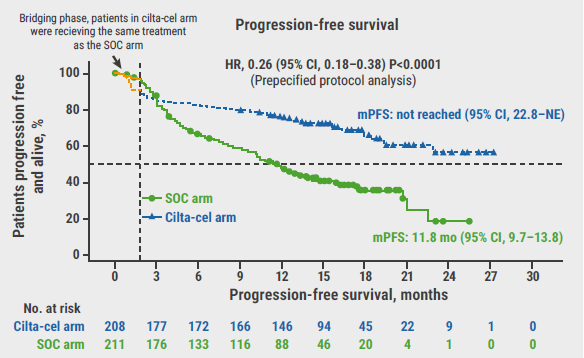
Immunotherapies have started moving to earlier lines of therapy. The phase 3 CARTITUDE-6 trial (NCT05257083) assesses ciltacabtagene autoleucel (cilta-cel) compared with autologous stem cell transplant (ASCT) in participants with newly diagnosed multiple myeloma who received daratumumab, bortezomib, lenalidomide, and dexamethasone (DVRd) induction [5]. Following cilta-cel or ASCT, all participants are to receive daratumumab-lenalidomide maintenance and will be followed up for sustained minimal residual disease (MRD) negativity and progression-free survival [5].
MajesTEC-5 (GMMG-HD10/DSMM-XX, NCT05695508) is another example trial of immunotherapy in early lines, enrolling participants with transplant-eligible newly diagnosed multiple myeloma. Assessed is the combination of teclistamab plus daratumumab-lenalidomide-dexamethasone (DRd) induction, followed by ASCT and maintenance with teclistamab plus daratumumab-lenalidomide (DR). “In this trial, there is an opportunity to discontinue therapy if patients achieve MRD negativity for 12 months or more and then continue with standard-of-care maintenance,” said Dr Mai.
MagnetisMM-6 (NCT05623020) is an open-label, multicentre, two-part, randomised, phase 3 trial. In the second part of the trial, participants with transplant-ineligible newly diagnosed multiple myeloma are randomised to either elranatamab plus DR or DRd [6]. According to Dr Mai, the DRd comparator arm was chosen because “this is the true standard-of-care that we use in clinical practice”.
The multicentre, open-label, phase 2 EMN34 trial (ERASMM, NCT06183489) investigates elranatamab treatment in participants with smouldering multiple myeloma who present with at least 2 high-risk features.
As therapies are now moving to earlier lines, “we need novel outcome measures such as sustained MRD negativity or combined endpoints, as many patients will experience prolonged PFS,” concluded Dr Mai. “Studies are needed to explore the limited duration of treatment and optimise dose schedules. Balancing efficacy and safety becomes more important, especially in low-risk multiple myeloma and early treatment.”
- Rafae A, et al. Oncologist. 2024;29(3):200-212.
- Mai EK. Moving immunotherapy in early lines. Session VII: Immunotherapy. EMN 2024, 18–20 April, Turin, Italy.
- Ailawadhi S, et al. Clin Lymphoma Myeloma Leuk. 2024;24(5):e217-e225.
- Gagelmann N, et al. J Clin Oncol. 2024:JCO2302232.
- Boccadoro M, et al. Blood (2022) 140 (Supplement 1): 4630–4632.
- Grosicki S, et al. J Clin Oncol. 2023;41(16_suppl):TPS8065.
Posted on

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com