
In colon cancer, TDs have been associated with worse prognosis. However, this marker is included in the TNM staging system only in the absence of lymph node metastasis (i.e., stage 3 pN1c tumours). Dr Romain Cohen (Mayo Clinic, USA) presented the prognostic value of TDs and addition of TDs in the count of lymph node metastases in patients with stage 3 colon cancer from the CALGB/SWOG 80702 phase 3 trial (NCT01150045) [1].
Pathology reports of evaluable patients (n=2,028) were reviewed for presence and count of TDs, primary tumour sidedness, lymphovascular invasion, and perineural invasion. Disease-free survival (DFS) and overall survival (OS) were evaluated by multi-variable Cox models adjusting for treatment arm, T-stage, N-stage, lymphovascular invasion, perineural invasion, and lymph node ratio.
Of the included patients, 524 (26%) were TD-positive and 1,504 (74%) were TD-negative. Of the TD-positive patients, 80 (15.4%) were node negative (i.e., pN1c), 239 (46.1%) were pN1a/b, and 200 (38.55%) were pN2; 17.2% and 37.0% of all pN1a/b and pN2 tumours had TDs. Overall median follow-up was 69.3 months. The presence of TDs was associated with poorer DFS (HR 1.59; 95% CI 1.28-1.91) and OS (HR 1.52; 95% CI 1.18-1.95). The negative effect of TD on these endpoints was observed for both pN1a/b and pN2 groups.
Among TD-positive patients, the number of TDs had a linear negative effect (see Figure). Adding TD to the count of lymph node metastases, 104/1,570 (6.6%) patients initially considered as pN1 were re-staged as pN2. Re-staged pN2 patients experienced worse DFS (3-year DFS rate: 65.5% vs 80.3%, P=0.0003) and OS (5-year OS rate 69.1% vs 87.8%; P=0.0005) than patients confirmed as pN1. Re-staged pN2 patients had similar DFS than patients initially staged as pN2 (3-year DFS rate: 65.5% vs 63.1%, P=0.1992). OS curves of these 2 groups crossed, with better outcomes during the first 3 years of follow-up, but poorer 5-year estimates for re-staged pN2 patients (5-year OS rate: 69.1% vs 74.8%, P=0.0436).
Figure: Linear effect of the number of TDs on disease-free survival [1]
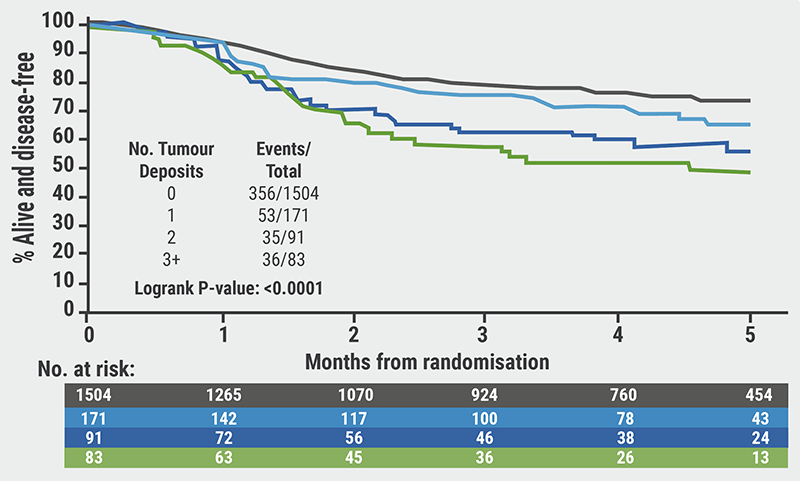
Dr Cohen summarised: “Tumour deposits are found in more than a quarter of stage 3 colon cancers. Tumour deposits should be considered as a quantitative barometer, since their number has an impact on patients' prognosis. By adding the number of tumour deposits to the count of lymph node metastases, we improve the prognostication accuracy of the TNM staging system.”
Copyright ©2021 Medicom Medical Publishers
Posted on

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com