
Dr Amitai Segev (Sheba Medical Centre, Israel) presented a study that retrospectively evaluated 16,432 patients aged ≤45 years who were admitted to the internal and cardiology wards at a large tertiary centre between January 2009 and December 2019 [1]. The purpose of the study was to identify the determinants of AF in this population to facilitate timely diagnosis, follow-up, and management.
Clinical, electrocardiographic (ECG), and echocardiographic data were collected and compared between participants with AF (n=366) and without AF (n=16,066) at baseline. A subgroup of participants without AF at baseline and a subsequent hospital visit were followed for the development of new-onset AF. Baseline characteristics of patients with AF were statistically significantly different from those without AF in a variety of parameters strongly and independently associated with young-onset AF, including age, male gender, obesity, and heart failure (see Table).
Table: Idependent predictors of new-onset AF. Adapted from [1]
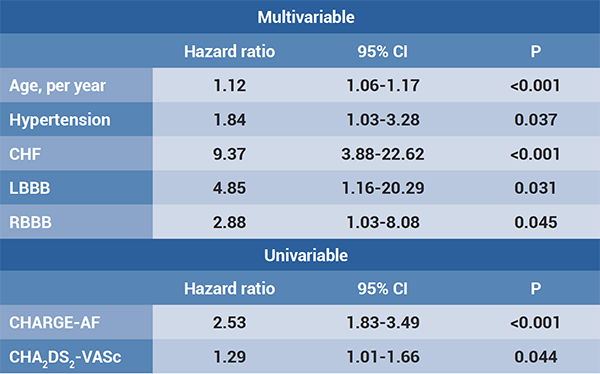 AF, atrial fibrillation; CHF, congestive heart failure; CI, confidence interval; LBBB, left bundle branch block; RBBB, right bundle branch block
AF, atrial fibrillation; CHF, congestive heart failure; CI, confidence interval; LBBB, left bundle branch block; RBBB, right bundle branch block Cox proportional hazards regression on determinants associated with new-onset AF.
A total of 10,691 participants were followed for a median of 41.5 (16.6-78.6) months, during which 85 patients developed new-onset AF (equivalent to 0.5%/year). Independent predictors of new-onset AF were increased age, hypertension, heart failure, and right and left bundle branch block (P≤0.045).
The analysis also compared 2 clinical scores in their ability to predict new-onset AF. The CHARGE-AF score is a validated clinical score incorporating readily available variables, such as age, ethnicity, lifestyle parameters, and cardiovascular comorbidities. The CHA2DS2-VASc score has originally been developed to predict the risk of stroke in AF. In this study, the CHARGE-AF score outperformed the CHA2DS2-VASc score in new-onset AF prediction (area under the ROC curve 0.75 [0.7-0.8] vs 0.56 [0.48-0.65], respectively).
In summary, young-onset AF is characterised by a specific clinical profile of comorbidities and ECG abnormalities. The incidence of new-onset AF in individuals admitted to hospital was 0.5%/year. Outcomes of this retrospective cohort study suggest that patients at high risk for the development of new-onset AF can be identified by clinical parameters and that more intense follow-up of selected individuals may result in early diagnosis, followed by early intervention.
- Segev A. Atrial fibrillation in the young: clinical characteristics, predictors of new onset and outcomes. EHRA 2021 Congress, 23-25 April.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: EHRA 2021
Featured articles
Atrial Fibrillation and Direct Oral Anticoagulant
Predictors of young-onset atrial fibrillation
RACE 3 long-term results show fading benefit of targeted therapies in AF and HF
Deep dive into EAST-AFNET 4 results on early rhythm-control in atrial fibrillation
Cryo-FIRST study: improved AF and QoL outcomes with cryoballoon versus drug therapy
STROKESTOP: Benefits of systematic screening for atrial fibrillation
DOACs and bleeding: the role of antidotes
2021 EHRA practical guide: DOACs in pre-operative and bleeding patients
Atrial Ablation
Early rhythm-control ablation: insight from the CHARISMA registry
Personalised pulmonary vein isolation procedure feasible and effective
Pulmonary vein isolation: cryoballoon non-inferior to radiofrequency ablation
Diagnostic Tools
EHRA Practical Guide on cardiac imaging in electrophysiology
Novel diagnostic score accurately differentiates between athlete’s heart and ARVC
The precordial R-prime wave: a discriminator between cardiac sarcoidosis and ARVC
Limited added value of ECG-based mortality prediction in COVID-19 patients using machine learning
Devices
EHRA expert statement on pacemakers and intracardial devices: “watch out for the little old lady”
5-Year efficacy of subcutaneous implantable cardioverter defibrillator
Specific Populations
Individualised approaches key to success in resynchronisation therapy non-responders
Antiarrhythmic drug treatment in children: evidence-based recommendations
The importance of cardiac imaging in patients with congenital heart disease
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy
HEAD OFFICE
Laarderhoogtweg 25
1101 EB Amsterdam
The Netherlands
T: +31 85 4012 560
E: publishers@medicom-publishers.com