In patients aged ≥50 years, GCA is the most prevalent form of primary vasculitis. Irreversible blindness occurs in up to 30% of the cases. Although high dose glucocorticoids are an effective treatment, toxicity is a major problem and occurs in over 80% of patients. Therefore, a correct diagnosis and accurate monitoring of the disease are important. In prior studies, a non-compressible halo sign of the temporal and axillary arteries has demonstrated discriminative value for diagnosing GCA [2].
The current 2-centre, prospective study aimed to assess the potential of ultrasound for monitoring newly diagnosed GCA patients by analysing the sensitivity to change of ultrasound halo characteristics, and their connection to disease activity and glucocorticoid therapy. To this end, ultrasound features of patients with clinical relapse were assessed. A total of 49 patients with ultrasound-confirmed GCA (mean age 78.2, 73.5% women) were included in the study. The sensitivity of halo to change was calculated by the mean difference of halo features (non-standardised variation) between baseline and the different timepoints (1, 3, 6, 12, and 24 weeks). Dr Cristina Ponte (Hospital de Santa Maria Lisbon, Portugal) shared the results of the study.
The sum of all arterial segments with halo –temporal and axillary arteries combined– demonstrated halo sensitivity to change over 24 weeks at all timepoints compared with baseline. The sum of halo intima-media thickness (IMT) demonstrated sensitivity to change at these timepoints as well. When temporal and axillary arteries were evaluated separately, only the sum of temporal arterial segments with halo and accessory IMT were sensitive to change at all timepoints (see Figure).
Figure: Halo sensitivity to change during disease follow-up [1]
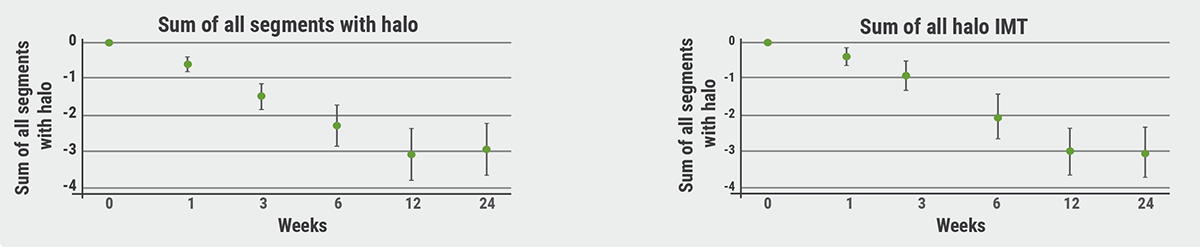
IMT, intima-media thickness.
A significant association was found between the sum of all segments with halo and disease activity as measured by erythrocyte sedimentation rates, C-reactive protein, and Birmingham Vasculitis Activity Score (all P<0.05). Corresponding correlations for the sum of axillary halo segments and ESR, CRP, and BVAS were not significant. Correlations were similar for the sum of IMT of the separate arteries. In addition, a significant correlation was found between glucocorticoid cumulative dose and the sum of temporal segments with halo (-0.34; P<0.05). The sum of all segments with halo was related to the probability of being in disease remission, defined as an absence of relapse plus prednisone dose <30 mg/day (OR 0.47). Halo sign features of temporal segments were also associated with the probability of being in disease remission (OR 0.39). Finally, the sum of all segments with halo (P=0.0012) and temporal segments with halo (P=0.0012) were predictive of relapse. Dr Ponte concluded that ultrasound is a valuable tool in the monitoring of GCA patients: “A composite score of halo size and extent could be used to assess disease activity and treatment response in GCA patients.”
- Ponte C, et al. Ultrasound halo sign as a potential monitoring tool for patients with giant cell arteritis: a prospective analysis. OP0055, EULAR 2021 Virtual Congress, 2–5 June.
- Dejaco C, et al. Ann Rheum Dis 2018;77(5):636-43.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: EULAR 2021
Featured articles
COVID-19 Update
Rituximab or JAK inhibitors increase the risk of severe COVID-19
Updates on COVID-19 vaccines in patients with rheumatic disease
Immunomodulatory therapies for severe COVID-19: literature update
New Developments in Rheumatoid Arthritis
JAK inhibitors and bDMARDs not associated with increased risk of serious infections in RA
Remote management of RA is a feasible alternative for outpatient follow-up
TOVERA: Ultrasound is a promising biomarker of early treatment response
The risks of polypharmacy in RA
ABBV-3373: A potential new therapeutic agent for RA
JAK inhibitors and bDMARDs show comparable effectiveness
Spondyloarthritis: Progression in Therapies
SELECT-AXIS: 64-week results of upadacitinib in active ankylosing spondylitis
Guselkumab efficacious in PsA patients with inadequate response to TNF inhibition
Faecal microbiota transplantation not effective in active peripheral PsA
Risankizumab meets primary and ranked secondary endpoints in PsA
Prognostic factors for minimal disease activity in early psoriatic arthritis revealed
Imaging in Large-Vessel Vasculitis
PET/CT is a reliable measure of disease activity in LVV, but does not predict future relapses
Ultrasound is useful for disease monitoring in giant cell arteritis
Prevention in Rheumatic Diseases
Air pollution predicts decreased response to biological treatment in rheumatic diseases
Passive smoking associated with an increased risk of RA
Gene-Environment Interaction in Gout
Gene-diet and gene-weight interactions associated with the risk of gout
What Is New in Systemic Lupus Erythematosus
Intensified treatment regimen of anifrolumab for lupus nephritis is promising
Systemic lupus erythematosus: increased risk of severe infection
Juvenile Idiopathic Arthritis and Osteoarthritis
Efficacy and safety of secukinumab in juvenile idiopathic arthritis
Emerging therapies and future treatment directions in osteoarthritis
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy