“First-line options for patients with uHCC have been limited, with sorafenib and lenvatinib being the main options,” Prof. Ghassan Abou-Alfa (Memorial Sloan Kettering Center, NY, USA) said. “These agents have been associated with a median OS of approximately 1 year and quality-of-life reducing toxicity.” Recently, atezolizumab and bevacizumab outperformed sorafenib [2]. Also, tremelimumab, a CTLA-4 inhibitor, plus durvalumab, a PD-L1 inhibitor, showed promising activity in this population in a phase 2 trial [3].
The current open-label, multicentre, phase 3 HIMALAYA trial (NCT03298451) randomised patients with uHCC 1:1:1 to tremelimumab 300 mg single dose plus durvalumab 1,500 mg every 4 weeks (T300+D regimen; n=393), durvalumab monotherapy (n=389), or sorafenib 400 mg twice daily (n=389). The primary objective was to compare the T300+D regimen with sorafenib regarding OS.
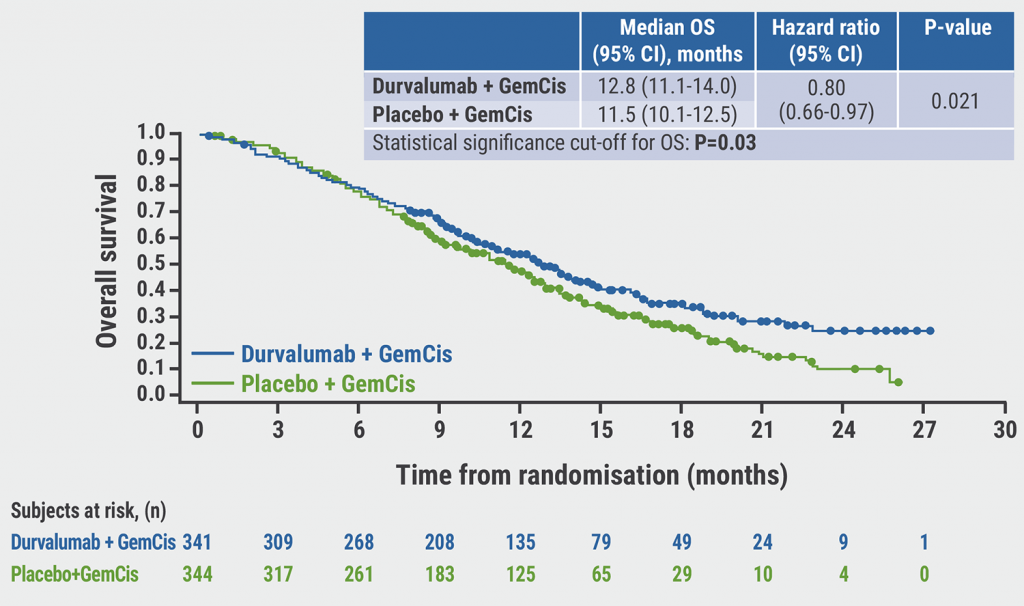
T300+D was superior to sorafenib in terms of median OS (16.4 vs 13.8 months; HR 0.78; P=0.0035). The OS difference between the 2 treatment regimens increased over time: 18-month OS rates were 48.7% and 41.5%; 36-month OS rates were 30.7% and 20.2% (see Figure). The superiority of T300+D over sorafenib was consistent across subgroups. Furthermore, the median OS for patients on durvalumab monotherapy was non-inferior to that of patients in the sorafenib arm (16.6 vs 13.8 months; HR 0.86).
Figure: Overall survival of T300+D versus sorafenib [1]

The safety profiles of the novel treatment regimens were manageable. Grade 3 or 4 adverse events (AEs) occurred in 25.8%, 12.9%, and 36.9% of the patients on T300+D, durvalumab monotherapy, and sorafenib, respectively. Hepatic or haemorrhagic SMQ events were limited in the T300+D arm, with 7.0% and 0.5% grade 3 or higher events in this treatment arm. The prevalence of immune-mediated AEs met the expectations of the authors. The most common grade 3 or 4 AEs in the T300+D and durvalumab arms were hepatic events (4.1%, 4.4%), diarrhoea (3.6%, 0.3%), and dermatitis/rash (1.8%, 0.3%).
In conclusion, the authors suggested that durvalumab ± tremelimumab is a possible new standard for patients unable to receive bevacizumab.
- Abou-Alfa GK, et al. Phase 3 randomized, open-label, multicenter study of tremelimumab and durvalumab as first-line therapy in patients with unresectable hepatocellular carcinoma: HIMALAYA. Abstract 379, ASCO GI 2022, 20–22 January.
- Finn RS, et al. N Engl J Med 2020;382:1894–1905.
- Kelley RK, et al. J Clin Oncol. 2021;39(27):2991–3001.
Copyright ©2022 Medicom Medical Publishers
Posted on
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy