Since February 2021, several cases of unusual thrombotic events in combination with thrombocytopenia were observed in people who received AstraZeneca’s nCov-19 vaccine. Prof. Andreas Greinacher (Universitätsmedizin Greifswald, Germany) presented previously published and unpublished data on VITT [1].
The typical VITT pattern is development of thrombocytopenia, cerebral vein, and/or splanchnic vein thrombosis 4–20 days after vaccination with an adenoviral vector-based SARS-CoV-2 vaccine, strongly positive results for platelet factor 4 (PF4)/heparin IgG ELISA, and Fc-gamma receptor-mediated platelet activation in presence of PF4 [2–5].
The current hypothesis of the mechanism of VITT is as follows: early stage (days 1–2) consists of 2 parts, namely antigen formation of PF4/vaccine complexes and danger signalling by vaccine-induced inflammation; in late stage (days 5–14), highly pathogenic anti-PF4 antibodies are produced in high titres, which induce platelet activation and NETosis, leading to prothrombotic state, amplification, and loss of control [1].
The complex formation theory was supported by dynamic light scattering analysis of ChAdOx1 nCOV-19, with the particles being approximately 90 nm long (corresponding to the size of adenovirus). Then, VITT-patient affinity-purified anti-PF4 was added, which significantly increased the size of particles. When DNA was added, complexes increased to approximately 750 nm in size.
The co-inflammatory signal is suggested to come from the HEK cell line in which the vaccine is raised, and which contributes to approximately 50% of protein content (17.5–20 µg) per vaccine dose. Thus, there are many free hexon proteins in the vaccine, which are strong triggers of the innate immune system. Another factor might be EDTA-induced vascular leakage, which allows vaccine components to enter the vasculature at injection site, adding strong pro-inflammatory effects.
Prof. Greinacher also hypothesised that the HEK-cell protein in the vaccine may cause the formation of alloantibodies, which may then induce thrombocytopenia. This is supported by a vaccine-induced foetomaternal incompatibility causing pancytopaenia due to alloantibody formation in cattle and should be investigated further [1,6].
In summary, VITT is caused by anti-PF4 antibodies. Human and free proteins, and EDTA in the vaccine likely trigger the immune response to PF4. Anti-PF4 autoantibodies activate platelets, which recruit granulocytes, which then get into NETosis. This amplifies the reaction and causes a thrombin burst. It remains unclear whether the vaccine induces immune responses against other proteins.
- Greinacher A. Vaccine associated thrombotic thrombocytopenia. EHA 2021 Virtual Congress, 9–17 June:p217-3
- Greinacher A, et al. N Engl J Med 2021; 384:2092–101.
- Schulz NH, et al. N Engl J Med 2021; 384:2124–30.
- Scully M, et al. N Engl J Med 2021; 384:2202–11.
- Muir KL, et al. N Engl J Med 2021; 384:1964–5.
- Bastian M, et al. Vaccine 2011;29(32):5267–75.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: EHA 2021
Featured articles
Lymphoma
Immuno-oncology agents are effective in treating classic Hodgkin’s lymphoma
MATRix with ASCT: best long-term survival for primary CNS lymphoma
Naratuximab emtansine + rituximab safe and effective in diffuse large B-cell lymphoma
The journey ahead for CAR T-cell therapy in r/r follicular lymphoma
ZUMA-5 vs SCHOLAR-5: Axicabtagene ciloleucel significantly improves FL outcome
Promising chemo-free treatment options in r/r DLBCL
Leukaemia
Sabatolimab achieved durable responses in patients with high-risk MDS and AML
Final analysis of EURO-SKI: primary endpoints met in chronic myeloid leukaemia
Favourable outcomes with zanubrutinib versus ibrutinib in patients with r/r CLL
Oral azacitidine improves overall survival in patients with acute myeloid leukaemia
Reduced-intensity conditioning ASCT is effective in older patients with AML
ELEVATE-TN: Acalabrutinib shows long-term efficacy in chronic lymphocytic leukaemia
ELEVATE-RR: Acalabrutinib demonstrates similar efficacy and better safety versus ibrutinib
Fixed 12 cycles and MRD-guided venetoclax consolidation effective in CLL
GLOW: Ibrutinib + venetoclax showed superior PFS as first-line CLL treatment
Myeloma and Myelofibrosis
Novel targets in myelofibrosis: overview of emergent therapies
Immune therapy of multiple myeloma
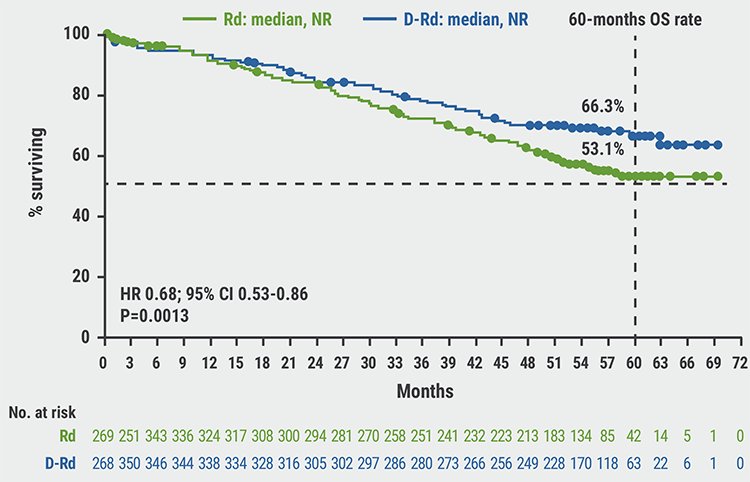
MAIA results confirm superior efficacy of daratumumab with standard-of-care
ANDROMEDA: Addition of daratumumab showed superior efficacy in patients with AL amyloidosis
Thrombotic and Thrombocytopenic Disorders including COVID-19 related
Acquired TTP: new treatments and updated guidelines
Maternal screening to prevent foetal and neonatal alloimmune thrombocytopenia
Fostamatinib effectively increased platelet counts in immune thrombocytopenic purpura
Physiopathology of coagulopathy in haematological malignancies and COVID-19
Haemostatic abnormalities are associated with mortality in COVID-19
Mechanisms of COVID-19 vaccine-induced thrombotic thrombocytopenia
COVID-19 vaccine-induced immune thrombotic thrombocytopenia: discovery and diagnosis
Haemoglobinopathies
Luspatercept improved anaemia in patients with non-transfusion-dependent β-thalassaemia
Personalising treatment for sickle cell disease
Gene therapy: A promising approach for hereditary haemoglobinopathies

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy