Prof. Noopur Raje (Massachusetts General Cancer Center and Harvard Medical School, USA) presented an overview on targeted immune stimulation therapies in multiple myeloma (MM) [1]. Multiple treatments are currently under development or were recently approved that harness the immune system and specifically redirect T cells.
One such exciting target in MM is B-cell maturation antigen (BCMA), an antigen expressed on plasma and myeloma cells, with higher expression on the latter. BCMA promotes myeloma cell growth and immunosuppression in the bone marrow [2]. Serum BCMA is elevated in MM and correlates with disease status and decreased survival, and many different immunotherapies are being developed: BCMA-CAR-T cells, BCMA-ADC (antibody-drug conjugate), and BCMA-TCE (T-cell engagers) [3].
One of the TCEs is CC-93269, a humanised IgG1-based TCE that binds to BCMA on myeloma cells and to CD3 on T cells, enabling specific and tight binding. CC-93269 was efficacious in animal models and primary patient bone marrow aspirates [4,5]. Preliminary results of a phase 1, dose-finding study (NCT03486067) in 30 patients with relapsing or refractory (r/r) MM showed an overall response rate (ORR) of 43.3% with 16.7% achieving a complete response (CR) [6]. Patients receiving 10 mg CC-93269 (n=9) showed an ORR of 88.9% with a CR of 44.4%, indicating a dose-response relationship. The median time to response was 4.1 weeks. Adverse events occurred in 73.3% of patients, and cytokine release syndrome (CRS) in 76.7%.
Teclistamab is a humanised BCMA x CD3 bi-specific IgG4 antibody. Prof. Raje presented updated results from an ongoing phase 1 study (NCT03145181; n=149) [7]. Preliminary efficacy data showed a dose-dependent ORR of 73% and CR of 23% with 1.5 mg/kg (high dose; n=22) after a median follow-up of 6.5 months. Responses were durable and deepened over time. CRS was recorded in 82 out of 149 patients, and there were no treatment discontinuations due to CRS events. PF-06863135, another bi-specific antibody candidate, showed a similar response rate of 80% in 20 participants in a phase 1 trial (NCT03269136) [8].
CAR T-cell therapy is an option for MM. Recently, idecabtagene vicleucel was approved after the KarMMa phase 2 pivotal study (NCT03361748) in patients with r/r MM (n=128) [9]. One dose of 300–460 x 106 cells led to an ORR of 73%, with a median duration of response of 10.9 months. After a median follow-up of 24.8 months, median PFS was 8.6 months and median OS was 24.8 months. The benefit-risk profile was favourable and supports its role as a treatment option for heavily pre-treated r/r MM.
Ciltacabtagene autoleucel is another CAR T-cell therapy, which is being investigated in the CARTITUDE-1 phase 1b/2 trial (NCT03548207) in r/r MM patients who were refractory to all prior lines of treatment (n=97) [10]. The overall response rate was 93% and after a median follow-up duration of 12.4 months, median PFS has not been reached.
The UNIVERSAL study (NCT04093596) is the first-in-human trial of allogeneic CAR T-cell therapy in patients with r/r MM (n=35) [11]. Preliminary data showed an ORR of ≤67%, with 6 out of 9 patients in the high-dose groups remaining in response. Toxicity was easy to manage.
Prof. Raje concluded, “Targeting BCMA is the new standard. Efficacy of CAR T-cells seems to be high, and toxicity is well manageable. Next steps will include strategies to combine or sequence these therapies, and next-generation approaches will focus on improving efficacy and duration of response.”
- Raje N. Targeted immune stimulation in myeloma: Immuno- and cellular therapies. 3SS133-SL4, EHA 2021 Virtual Congress, 09–17 June.
- Cho SF, et al. Front Immunol 2018;9:1821.
- Sanchez E, et al. Br J Haematol 2012;158(6):727–38.
- Seckinger A, et al. Cancer Cell 2017;31(3):396–410.
- Vu MD, et al. Blood 2015;128:2998.
- Costa LJ, et al. Abstract S205, EHA 2020, 11–21 June.
- Garfall AL, et al. Abstract 180, ASH 2020, 5–8 December.
- Lesokhin AM, et al. Abstract 3206, ASH 2020, 5–8 December.
- Anderson LD, et al. Abstract 8016, ASCO 2021, 4–8 June.
- Berdeja JG, et al. J Clin Oncol 2020;38:8505.
- Mailankody S, et al. Blood 2020;136(Suppl. 1):24-25.
Copyright ©2021 Medicom Medical Publishers
Posted on
Table of Contents: EHA 2021
Featured articles
Lymphoma
Immuno-oncology agents are effective in treating classic Hodgkin’s lymphoma
MATRix with ASCT: best long-term survival for primary CNS lymphoma
Naratuximab emtansine + rituximab safe and effective in diffuse large B-cell lymphoma
The journey ahead for CAR T-cell therapy in r/r follicular lymphoma
ZUMA-5 vs SCHOLAR-5: Axicabtagene ciloleucel significantly improves FL outcome
Promising chemo-free treatment options in r/r DLBCL
Leukaemia
Sabatolimab achieved durable responses in patients with high-risk MDS and AML
Final analysis of EURO-SKI: primary endpoints met in chronic myeloid leukaemia
Favourable outcomes with zanubrutinib versus ibrutinib in patients with r/r CLL
Oral azacitidine improves overall survival in patients with acute myeloid leukaemia
Reduced-intensity conditioning ASCT is effective in older patients with AML
ELEVATE-TN: Acalabrutinib shows long-term efficacy in chronic lymphocytic leukaemia
ELEVATE-RR: Acalabrutinib demonstrates similar efficacy and better safety versus ibrutinib
Fixed 12 cycles and MRD-guided venetoclax consolidation effective in CLL
GLOW: Ibrutinib + venetoclax showed superior PFS as first-line CLL treatment
Myeloma and Myelofibrosis
Novel targets in myelofibrosis: overview of emergent therapies
Immune therapy of multiple myeloma
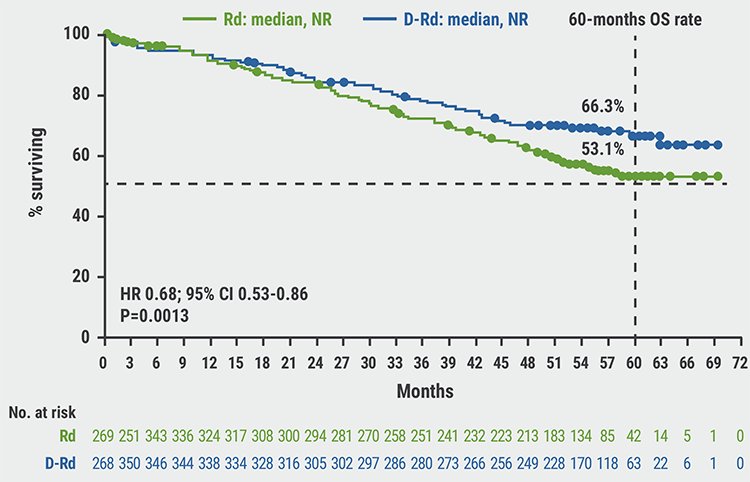
MAIA results confirm superior efficacy of daratumumab with standard-of-care
ANDROMEDA: Addition of daratumumab showed superior efficacy in patients with AL amyloidosis
Thrombotic and Thrombocytopenic Disorders including COVID-19 related
Acquired TTP: new treatments and updated guidelines
Maternal screening to prevent foetal and neonatal alloimmune thrombocytopenia
Fostamatinib effectively increased platelet counts in immune thrombocytopenic purpura
Physiopathology of coagulopathy in haematological malignancies and COVID-19
Haemostatic abnormalities are associated with mortality in COVID-19
Mechanisms of COVID-19 vaccine-induced thrombotic thrombocytopenia
COVID-19 vaccine-induced immune thrombotic thrombocytopenia: discovery and diagnosis
Haemoglobinopathies
Luspatercept improved anaemia in patients with non-transfusion-dependent β-thalassaemia
Personalising treatment for sickle cell disease
Gene therapy: A promising approach for hereditary haemoglobinopathies
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy