Brain metastases are often seen in treatment-naïve patients with stage 4 ROS1+ NSCLC, and the CNS is a common first site of progression [7]. Crizotinib is the only agent approved for treatment of patients with stage 4 ROS1+ NSCLC. However, preclinical data indicate that entrectinib is a more potent ROS1 inhibitor than crizotinib [8]. Entrectinib is a selective oral ROS1/NTRK/ALK TKI with activity in the CNS [8]. Designed to cross the blood-brain barrier and remain in the CNS, it is clinically active in primary brain tumours and secondary CNS metastases.
Doebele et al. conducted an integrated analysis of three phase 1/2 studies—STARTRK-2 [9]; STARTRK-1 [10], and ALKA-372-001 [10]. Enrolled patients had locally advanced or metastatic solid tumours. The safety-evaluable population included patients who had received ≥1 dose of entrectinib. The efficacy analysis included those with ROS1+ NSCLC and identified ROS1 fusions. Tumours were assessed at the end of cycle 1 and every 8 weeks thereafter. Primary endpoints were ORR and DoR (blinded independent central review [BIRC]; RECIST v1.1). Secondary endpoints were PFS and OS; intracranial ORR and DoR in patients with or without measurable CNS lesions at baseline; and safety and tolerability.
The efficacy analyses included 53 patients with treatment-naïve ROS1+ NSCLC. BIRC-determined ORR was 77.4%, with clinical response in 3 patients (5.7%). Median BIRC DoR was 24.6 months. Per baseline CNS status, median BIRC PFS was 26.3 months for patients without CNS disease (n=30) and 13.6 months for those with CNS metastases (n=23). Intracranial ORR was 55.0% and the median intracranial DoR was 12.9 months in patients with baseline CNS disease. The median for entrectinib had not been reached. Most treatment-related AEs in the overall safety cohort (n=355) were grade 1-2. Entrectinib was tolerable, with a manageable safety profile. Data show a robust systemic response in patients with ROS1+ NSCLC treated with entrectinib compared with crizotinib [7]. Outcomes suggest that those with ROS1 tumours may benefit from first-line use of a CNS-penetrant ROS1 inhibitor.
- Patil T, et al. J Thorac Oncol 2018.
- Rolfo C, et al. Expert Opin Investig Drugs 2015;24:1493-1500.
- STARTRK-2. NCT02568267.
- Drilon A, et al. Cancer Discov 2017;7:400-409.
Posted on
Table of Contents: WCLC 2018
Featured articles
Interview with the IASCL President, Dr. Giorgio Scagliotti
Presidential Symposium – Top 5 abstracts
Durvalumab after chemoradiotherapy extends OS in stage 3, unresectable non-small-cell lung cancer
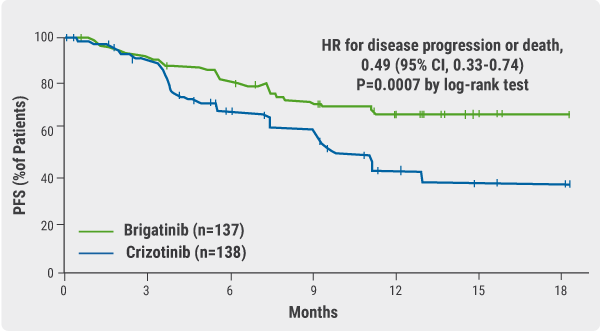
Potential for brigatinib as a first-line treatment option for ALK+ non-small-cell lung cancer
Benefits of chest CT screening
New standard of care in extensive-stage small-cell lung cancer
No progression-free survival benefit with nintedanib plus pemetrexed/cisplatin for malignant pleural mesothelioma of epithelial subtype
New Aspects of Immunotherapy
Next generation immunotherapy in non-small-cell lung cancer
Combination therapies: Where are we in 2018?
Choice of taxane and addition of pembrolizumab for metastatic squamous non-small-cell lung cancer
New Aspects of Targeted Therapy
PD-L1 expression in untreated EGFR-mutant non-small-cell lung cancer and response to osimertinib
Mesothelioma
Unmet needs in surgical management of malignant pleural mesothelioma
Advanced Non-small Cell Lung Cancer
Novel Therapies in ROS1 and EGFR
Advances in Small-cell and Neuroendocrine Tumours

site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy