Upadacitinib, an oral, reversible, Janus kinase (JAK) inhibitor approved for the treatment of rheumatoid arthritis, is currently under evaluation for treatment of psoriatic arthritis. The SELECT-PsA-1 study, presented by Prof. Iain McInnes (University of Glasgow, Scotland), assessed the efficacy and safety of upadacitinib compared with placebo and adalimumab in patients with psoriatic arthritis and prior inadequate response or intolerance to ≥1 non-bDMARD.
Participants (n=1,704) were randomised to 15 mg upadacitinib once daily, 30 mg upadacitinib once daily, 40 mg adalimumab every other week, or placebo. The primary endpoint of the study was the proportion of patients achieving American College of Rheumatology (ACR)20 for upadacitinib versus placebo at week 12. The mean age of the participants was 50.8 years, 53.2% were female, the mean duration of psoriatic arthritis diagnosis was 6.1 years, and 82% were on ≥1 concomitant non-bDMARD (84% received methotrexate ± another non-bDMARD).
At week 12, ACR20 rates were 70.6% in the 15 mg upadacitinib arm and 78.5% in the 30 mg upadacitinib arm, compared with 36.2% in the placebo group, and 65.0% with 40 mg adalimumab. A greater proportion of patients achieved ACR50/70 with 15 mg or 30 mg upadacitinib compared with placebo, and with 30 mg upadacitinib versus adalimumab (see Figure).
Figure: Efficacy outcomes SELECT-PsA-1 [1]
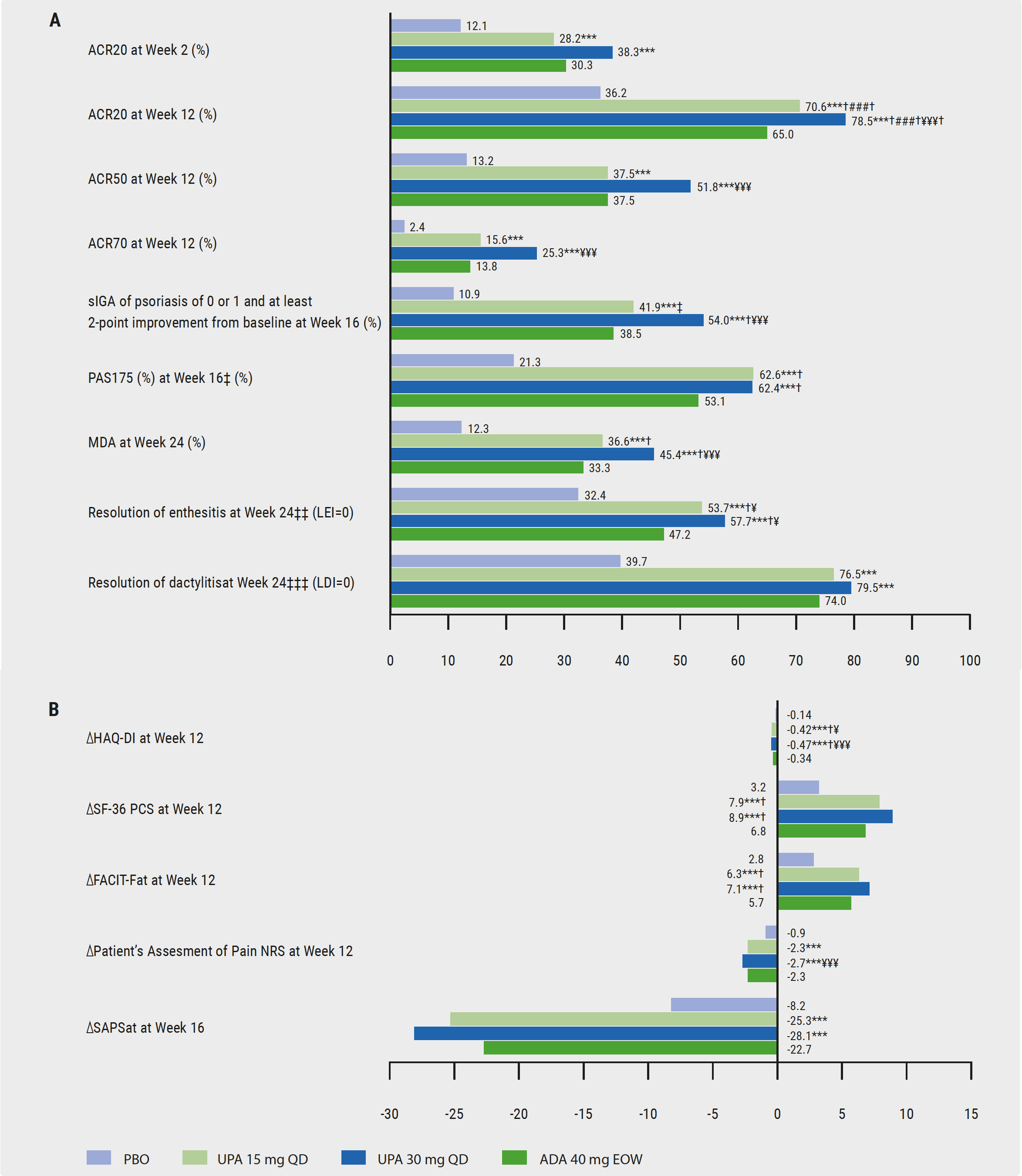 ADA, adalimumab; EOW, every other week; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI, Health Assessment Questionnaire Disability; LEI, Leeds Enthesitis Index; LDI, Leeds Dactylitis Index; MDA, minimal disease activity; PBO, placebo; PASI, Psoriasis Area Severity Index; SAPS, Self-Assessment of Psoriasis Symptoms; SF-36, Short Form Health Survey; s-IGA, static Investigator Global Assessment; UPA, upadacitinib; QD, once daily.‡ For participants with ≥3% body surface area psoriasis at baseline; ‡‡ for participants with LEI>0; ‡‡‡ for subjects with LDI>0.*** P<0.001 upadacitinib vs placebo; ** P<0.01 upadacitinib vs placebo; ### P<0.001 for non-inferiority upadacitinib vs adalimumab; ¥¥¥ P<0.001 upadacitinib vs adalimumab; ¥ P<0.05 upadacitinib vs adalimumab.† Statistically significant in the multiplicity-controlled analysis. Nominal P-value is provided for ACR50/70 at week 12 and ACR20 at week 2.
ADA, adalimumab; EOW, every other week; FACIT-F, Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI, Health Assessment Questionnaire Disability; LEI, Leeds Enthesitis Index; LDI, Leeds Dactylitis Index; MDA, minimal disease activity; PBO, placebo; PASI, Psoriasis Area Severity Index; SAPS, Self-Assessment of Psoriasis Symptoms; SF-36, Short Form Health Survey; s-IGA, static Investigator Global Assessment; UPA, upadacitinib; QD, once daily.‡ For participants with ≥3% body surface area psoriasis at baseline; ‡‡ for participants with LEI>0; ‡‡‡ for subjects with LDI>0.*** P<0.001 upadacitinib vs placebo; ** P<0.01 upadacitinib vs placebo; ### P<0.001 for non-inferiority upadacitinib vs adalimumab; ¥¥¥ P<0.001 upadacitinib vs adalimumab; ¥ P<0.05 upadacitinib vs adalimumab.† Statistically significant in the multiplicity-controlled analysis. Nominal P-value is provided for ACR50/70 at week 12 and ACR20 at week 2.At week 24, change in modified Sharp/van der Heijde score (mTSS) was +0.25 for placebo, -0.04 for 15 mg upadacitinib 15 mg, +0.03 for upadacitinib 30 mg, and +0.01 for adalimumab [1]. Rates of treatment-emergent adverse events (AEs) and serious AEs were similar in the groups receiving placebo, 15 mg upadacitinib, and adalimumab; they were higher in patients receiving 30 mg upadacitinib. However, the safety profile was in line with what was already known from studies of upadacitinib in rheumatoid arthritis.
Posted on
Table of Contents: EULAR 2020
Featured articles
COVID-19 and inflammatory rheumatic disease: some key issues
Secukinumab monotherapy as efficient as adalimumab
AxSpA real-life remission rates higher on biologics
Olokizumab significantly improves RA features and patient-reported outcomes
Rheumatoid Arthritis
New nanoparticle promising future agent in RA
Olokizumab significantly improves RA features and patient-reported outcomes
Low DAS at 4 months predicts sustained DMARD-free remission
Ankylosing Spondylitis
Reduced maintenance dose of certolizumab pegol can be used in axSpA
Worse response axSpA patients to second TNFi versus first TNFi
AxSpA real-life remission rates higher on biologics
Certolizumab pegol reduces acute anterior uveitis in axial spondyloarthritis
TNF-α inhibitors improve bone mineral density in AS patients
Psoriatic Arthritis
Ixekizumab shows sustained improvements in pain and fatigue at 3 years
Adalimumab added to methotrexate yields better results in PsA than methotrexate escalatio
Upadacitinib provides fast onset of improvement in psoriatic arthritis
Secukinumab monotherapy as efficient as adalimumab
Osteoporosis and Osteoarthritis
Higher mortality risk with tramadol versus NSAIDs for osteoarthritis patients
Hydroxychloroquine not effective in patients with hand osteoarthritis
Positive effect denosumab on fall risk
Systemic Sclerosis and Systemic Lupus Erythematosus
Anifrolumab achieves rapid and durable BICLA-response
Subclinical myocardial involvement progresses in SSc patients
Composite endpoint CRESS for primary Sjögren’s syndrome
COVID-19
COVID-19 and inflammatory rheumatic disease: some key issues
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy