Prof. Séverine Vermeire (University Hospital Leuven, Belgium) presented the results of the VISIBLE 2 study of subcutaneous vedolizumab as maintenance treatment CD. The 644 participants received intravenous vedolizumab 300 mg at weeks 0 and 2 as induction therapy. At week 6, the 412 clinical responders were then randomised to receive 108 mg subcutaneous vedolizumab (n=275) or placebo (n=134) every 2 weeks for up to 52 weeks. The primary endpoint was clinical remission at week 52, defined as a Crohn’s disease Activity Index (CDAI) score ≤150.
The primary endpoint was achieved by 48.0% of patients on subcutaneous vedolizumab versus 34.3% on placebo (P=0.008). Enhanced clinical response (decrease of ≥100 in CDAI score) was not significantly different: 52.0% versus 44.8% (P=0.167; see Figure). Prof. Vermeire stated that “the high placebo response may be explained by the carry-over effect of induction therapy”. Among patients on concomitant corticosteroids at baseline (n=95 and n=44 in the respective treatment groups), 45.3% versus 18.2% achieved corticosteroid-free clinical remission. Of anti-TNF-naïve patients, 48.6% and 42.9% achieved clinical remission.
Figure. Primary and secondary endpoints of VISIBLE 2 (full analysis set) [1]
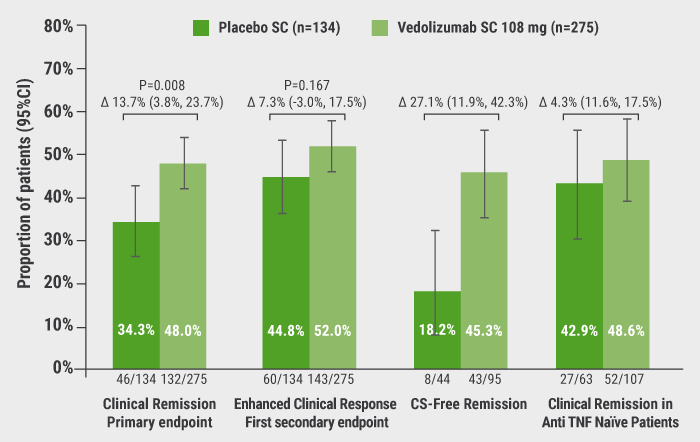
SC, subcutaneous; CS, corticosteroid
Less than 3% of patients treated with subcutaneous vedolizumab reported injection-site reactions. Serious infections, malignancy, and liver injury were seen in ≤5% in both arms. Numerically, serious infections were lower in the treatment group (n=4) versus placebo (n=6). Anti-vedolizumab antibodies were detected in 7 (2.5%) treated patients; 4 of 7 developed neutralising antibodies. There were no new safety signals.
- Vermeire S, et al. ECCO-IBD 2020, OP23.
Posted on
Table of Contents: ECCO 2020
Featured articles
Gut Microbiome as Treatment Target
Response to faecal microbiota transplantation in UC
Bioactives produced by gut bacteria to modulate immune response
Big Data Analysis
Multi-omics help describe CD phenotypes
The positive impact of genetic data on drug development
Experimental Therapies: Study Results
AMT-101: an oral human IL-10 fusion protein
Phase 2 results of first-in-class TL1A inhibitor
Open-label extension study of risankizumab: final results
Clinical remission after dose escalation of upadacitinib
Short- and Long-Term Treatment Results
Infliximab discontinuation increases relapse risk
Tofacitinib ‘real-world’ effectiveness in active UC
Subcutaneous ustekinumab as maintenance therapy in UC
Subcutaneous vedolizumab maintenance therapy in CD
Vedolizumab treatment persistence and safety
Specific Therapeutic Strategies
Impact of strategies on intestinal resection rate
Early ileocaecal resection in CD patients failing conventional treatment
Biologics before surgery in IBD do not elevate infection risk
Top-down infliximab superior to step-up in children with CD
High versus standard adalimumab in active UC
Head-to-Head Comparison of Treatments
Vedolizumab and anti-TNF therapies: a real-world comparison
Cancer Risk
Increased risk of small bowel cancer in IBD
Increased incidence of colorectal cancer and death in CD
Risk of rectal, anal cancer increased in perianal CD
Glyco-fingerprint as risk factor of UC-associated cancer
Miscellaneous Topics
Resolution of mucosal inflammation has dramatic effect
PICaSSO validated in real-life study
Re-inducing inflammation in organoids from UC patients
Role of immune cells in intestinal fibrosis
Association between meat consumption and IBD risk
CD exclusion diet corrects dysbiosis
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy