The suggested correlation between appendectomy and UC was investigated in a meta-analysis; at the same time, possible confounding factors were analysed.
A systematic review and meta-analysis were performed in July 2017 using MEDLINE, EMBASE and the Cochrane library. Data from studies describing the influence of appendectomy on colectomy rate and risk of CRC and/or HGD were extracted from published reports. Exclusion criteria were patients <18 years, non-UC, and animal studies.
A total of 891 studies were collected, of which 13 studies evaluating 73,323 UC patients were included (appendectomy n=2,859). All studies except one were rated as poor quality. Overall, colectomy rate in appendectomised and non-appendectomised patients was not significantly different (OR 1.21, 95% CI 0.84-1.75).
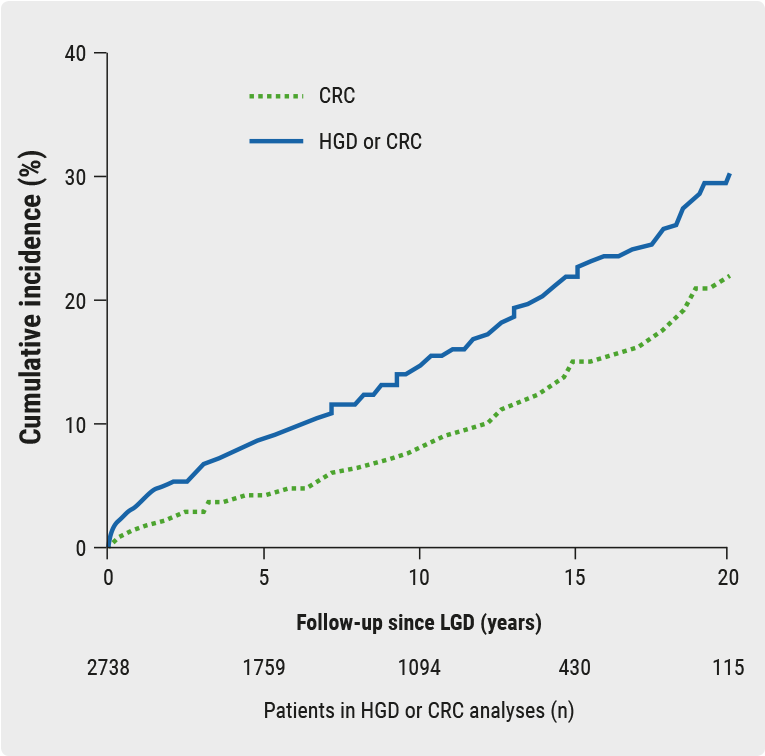
Four of six studies demonstrated significantly longer disease duration, however, with a decreased use of steroids after appendectomy. A total of six studies investigated the risk of CRC and/or HGD, which was significantly increased after appendectomy (OR 3.68, 95% CI 1.70-7.94).
Three studies looked at CRC specifically, which showed the same trend although not significantly so (OR 5.50, 95% CI 0.95-31.96). The increased incidence of malignant degeneration seemed related to longer disease duration. Average disease duration was 102.7 months in the appendectomy group vs. 76.6 months in the non-appendectomy group. Also, the cumulative percentage of primary sclerosing cholangitis was higher in appendectomised patients (13.7%) than in non-appendectomised patients (4.4%). Thus, a significantly increased risk of CRC and/or HGD after appendectomy in UC patients was found, which is presumably correlated with delayed colectomy.
This finding shows that there is no need to stop on-going trials, but emphasises the importance of endoscopic surveillance in high-risk patient groups [8].
- Stellingwerf ME, et al. DOP083. ECCO 2018.
Posted on
Table of Contents: ECCO 2018
Featured articles
IBD diagnostics
IBD disease patterns and genetics
Novel treatment strategies
Efficacy and safety of biologics
Oncology in IBD
Surgery for IBD
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy