Updated overall survival (OS) data from the phase 3 PACIFIC trial have set a new standard of care for first-line treatment of unresectable stage 3 NSCLC. Previously reported results showed that durvalumab significantly improved progression-free survival (PFS) by 11.2 months compared with placebo (HR 0.52; 95% CI 0.42-0.65; P<0.001) [1]. The latest findings show a 2-year landmark survival rate of 66.3% for patients in the durvalumab group vs 55.6% in the placebo arm (P=0.005). Dr Scott Antonia (H. Lee Moffitt Cancer Center and Research Institute, USA) reported results at the live session [2]. The study was simultaneously published in the New England Journal of Medicine [3].
PACIFIC was a randomised, double-blind, placebo-controlled trial. A total of 709 patients with locally advanced, stage 3, unresectable NSCLC underwent concurrent chemoradiotherapy with no progression after treatment. Patients with any PD-L1 tumour status were enrolled into the study and randomised to receive intravenous durvalumab (n=473; 10 mg/kg of body weight) or placebo (n=236) every 2 weeks for up to 12 months. Randomisation occurred up to 42 days after concurrent chemoradiotherapy and was stratified according to age, sex, and smoking history. Primary endpoints were PFS and OS. Durvalumab is a selective human IgG1 monoclonal antibody that blocks PD-L1 binding to PD-1 and CD80, allowing T-cells to recognise and kill tumour cells [4,5].
Updated results showed that durvalumab significantly improved OS vs placebo (stratified HR 0.68; P=0.00251). Although the median OS had yet to be reached for durvalumab, it was 28.7 months for patients in the placebo arm. The survival benefit was seen in all prespecified subgroups. The median PFS was 17.2 vs 5.6 months for durvalumab and placebo, respectively. Findings on secondary outcomes also favoured durvalumab over placebo. There were no new safety issues. An unplanned post-hoc analysis, showed that OS was shorter (HR 1.36) in patients with tumour PD-L1 expression ≤1% who received durvalumab, but the finding was not statistically significant. Noteworthy, the group was relatively small and imbalances in baseline characteristics existed. OS outcomes from the PACIFIC trial provide compelling evidence for the benefit of durvalumab as the standard of care for patients with unresectable, stage 3 NSCLC.
- Antonia SJ, et al. N Engl J Med 2017;377:1919-1929.
- Antonia SJ, et al. Abstract PL02.01. IASLC 19th WCLC. 23-26 September 2018, Toronto, Canada.
- Antonia SJ, et al. N Engl J Med 2018:DOI: 10.1056/NEJMoa1809697.
- Ibrahim R, et al. Semin Oncol 2015;42:474-483.
- Stewart R, et al. Cancer Immunol Res 2015;3:1052-1062.
Posted on
Table of Contents: WCLC 2018
Featured articles
Interview with the IASCL President, Dr. Giorgio Scagliotti
Presidential Symposium – Top 5 abstracts
Durvalumab after chemoradiotherapy extends OS in stage 3, unresectable non-small-cell lung cancer
Potential for brigatinib as a first-line treatment option for ALK+ non-small-cell lung cancer
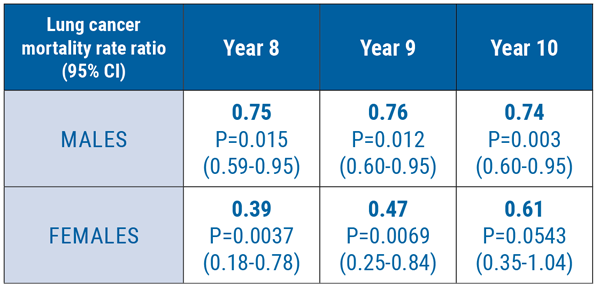
Benefits of chest CT screening
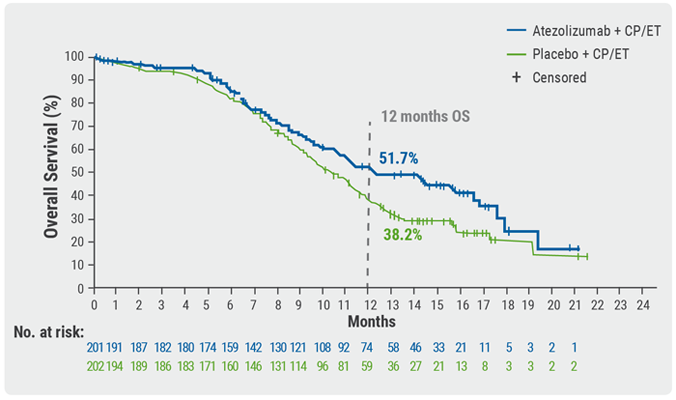
New standard of care in extensive-stage small-cell lung cancer
No progression-free survival benefit with nintedanib plus pemetrexed/cisplatin for malignant pleural mesothelioma of epithelial subtype
New Aspects of Immunotherapy
Next generation immunotherapy in non-small-cell lung cancer
Combination therapies: Where are we in 2018?
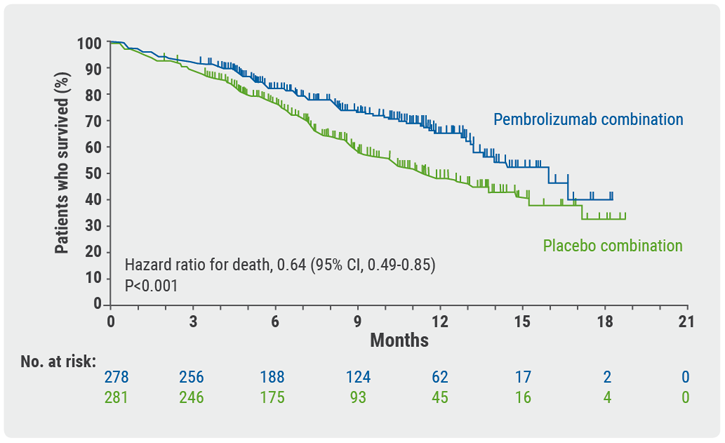
Choice of taxane and addition of pembrolizumab for metastatic squamous non-small-cell lung cancer
New Aspects of Targeted Therapy
PD-L1 expression in untreated EGFR-mutant non-small-cell lung cancer and response to osimertinib
Mesothelioma
Unmet needs in surgical management of malignant pleural mesothelioma
Advanced Non-small Cell Lung Cancer
Novel Therapies in ROS1 and EGFR
Advances in Small-cell and Neuroendocrine Tumours
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy