Genome-wide association studies implicated ligands for the Natural Killer Group 2D (NKG2D) receptor (a product of the KLRK1 gene) in disease pathogenesis [2]. In a murine model of AA, a type I cytotoxic pathway has been demonstrated as responsible for the disease state, with NKG2D-expressing CD8+ cytolytic T-lymphocytes necessary for the induction of the disease. Upregulation of IL-15 in the outer root sheath of the hair follicle activates cytolytic T-lymphocytes, which in turn produce Interferon (IFN)γ, leading to activation of the hair follicle and upregulation of IL-15, NKG2D ligands, and major histocompatibility complex (MHC) molecules, all of which target the hair follicle for attack [3].
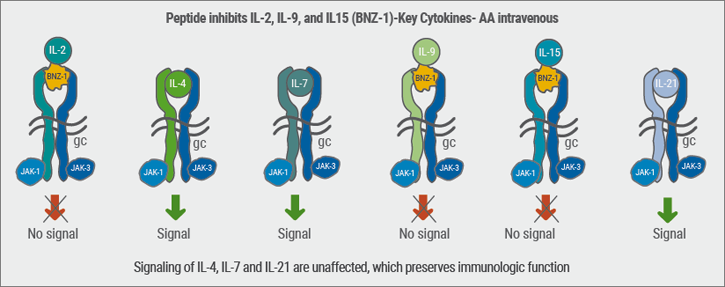
A possible therapeutic approach is the restoration of this immune privilege by restoring the defective function of CD4+/CD25+ cells and by reducing CD8 T lymphocytes and IL-15. JAK 1/3 signalling mediates IL-15 activation of T-lymphocytes [4]. IL-15 is highly expressed in human and murine AA and drives CD8 killer activation. IFN γ is a second important player in the AA pathogenesis: it is produced by killer T cells and drives inflammation. JAK inhibitors block both IL-15 and IFNγ.
A breakthrough in AA therapy was a publication in 2014 where, in a patient with plaque psoriasis, the oral JAK-inhibitor tofacitinib reversed alopecia universalis [5]. An open trial where AA was treated with oral tofacitinib confirmed that the majority of patients experience a regrowth of hair independent of age, disease severity, and disease duration with only minimal side effects [6]. 47% of patients experience a regrowth of hair by 12 months. In addition, the JAK inhibitor also improves nail dystrophy that was reported in 23% of patients. This and other work has spawned so much interest that there are now many JAK inhibitors in the clinical development for AA.
1. Bergfeld, W. Oral presentation session S048, AAD Annual Meeting, February 16–20 2018.
2. Xing, L. et al. Nat Med 2014;20:1043–9.
3. Jabbari, A. et al. J Invest Dermatol 2013;12:1395.
4. Ghoreschi, K. et al. J Immunol. 2011;186: 4234–43
5. Craiglow, BG. & King, BA. J Invest Dermatol 2014;134:2988–90.
6. Ibrahim, O. et al. JAMA Dermatol 2017;153:600–02.
Posted on
Table of Contents: AAD 2018
Featured articles
Letter from The Editor
Living in the golden age of psoriasis and atopic dermatitis therapies
Late-breakers
IL-17C inhibition in AD and new oral treatments
Dual JAK/SYK inhibitor and anti-IL-33 blockade
Psoriasis: Selective IL-23 blocker, analysis of VOYAGE-2, dual IL-17 inhibitor and ustekinumab
Hyperhidrosis: Soft molecule and anticholinergic towelettes
Behcet’s syndrome and hidradenitis suppurativa
Psoriasis: an update
Oral therapeutics, supersaturation and excimer laser
Psoriasis management online?
What's hot in atopic dermatitis
AD sleep disturbance, antihistamines and osteoporosis
New topical and systematic treatments
Acne management
Winter effect and preventing scarring
Restrictive antibiotic use and novel tetracycline
Alopecia Areata
Melanoma
Melanoma incidence continues to rise in Europe
Lesions in paediatric patients and possible correlation with coffee drinking
CNNs and targeted combination therapy
Pearls of the posters
Improvement in impact of genital psoriasis on sexual activity with use of ixekizumab
Intralesional cryosurgery and itching in psoriasis
site created by:

© 2024 Medicom Medical Publishers. All rights reserved. Terms and Conditions | Privacy Policy